Dr. Futterer notes that the clinical indications for prostate MRI in the 20th century initially was for locoregional staging. Specifically, this included using a phased array coil and 1.5T system to assess prostate anatomy. Moving past locoregional staging, we are now using mpMRI for detection, localization, characterization, risk-stratification, surveillance, assessment for recurrence, and image-guidance for biopsy, surgery, focal therapy, and radiation therapy. Subsequently, dynamic contrast-enhanced (DCE)-MRI was a very sensitive technique but had low specificity leading to false-positive findings. Furthermore, there was a lack of standardization for this modality. MR spectroscopy allowed for improved specificity for detecting prostate cancer versus BPH, however, it was a very time consuming and cumbersome technique, as well as difficulties with interpretation. Since then, functional MRI has improved diagnostic capabilities of detection and localization compared to anatomical MRI but did not have widespread acceptance.
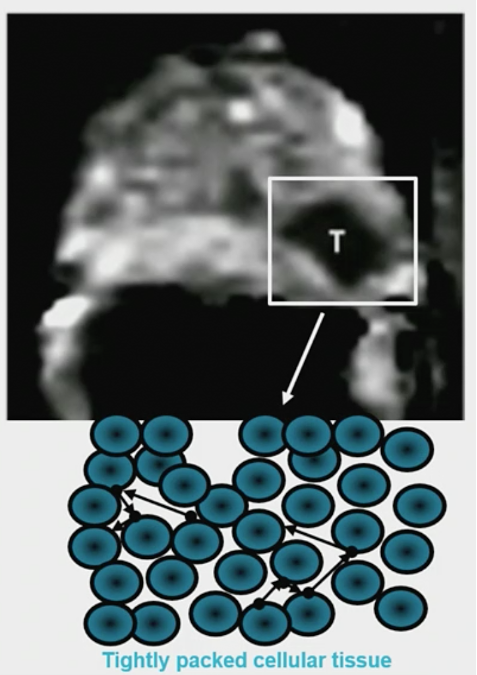
DWI is an essential component of mpMRI, which according to Dr. Futterer is the most important component of the mpMRI. DWI has high specificity for aggressiveness, but does have low spatial resolution and is susceptible to artifacts:
With DCE alone the area-under-the-curve (AUC) for detecting peripheral zone cancer is 0.72, whereas when adding DWI the AUC improves to 0.93.
Over the last several years, we have level 1 evidence suggesting we should use mpMRI prior to biopsy, based on the PRECISION,1 MRI-First2, and 4M3 studies. These outcomes are summarized in the following table:
Dr. Futterer notes that if we remove DCE, facilities are able to perform three MRIs per hour, forming the basis for the bpMRI and thus opening resources for performing more MRIs prior to a prostate biopsy. Furthermore, removing the coronal images and thus just performing axial images, decreases the timing of an MRI to 12 minutes (a so-called “fast” bpMRI). Several studies have compared bpMRI to mpMRI with generally similar accuracy for prostate cancer detection between the two modalities. In a study comparing mpMRI vs bpMRI vs fast bpMRI, sensitivity for high-grade prostate cancer for all protocols was 95% (180/190; 95% CI 91-97%).4 Specificity was 65% (285/436; 95% CI 61-70%) for fast bpMRI and 69% (299/436; 95% CI 64-73%) for bpMRI and mpMRI:
Dr. Futterer concluded his presentation with several take-home messages:
- Abbreviated MRI prostate protocols are appealing
- Considerations include indications, cost, experience, DWI artifacts, smart algorithms, and artificial intelligence
Presented by: Jurgen J. Futterer, MD, PhD, Intervental Radiologist, Radboud University Medical Center, Nijmegen, The Netherlands
References:
1. Kasivisvanathan V, Rannikko AS, Borghi M, et al. MRI-targeted or standard biopsy for prostate cancer diagnosis. N Engl J Med 2018;378(19):1767-1777.
2. Rouviere O, Renard-Penna R, Claudon M, et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naïve patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol 2019 Jan;20(1):100-109
3. van der Leest M, Cornel E, Israel B, et al. Head-to-head comparison of transrectal ultrasound-guided prostate versus multiparametric prostate resonance imaging with subsequent magnetic resonance-guided biopsy in biopsy-naïve men with elevated prostate-specific antigen: A Large Prospective multicenter study. Eur Urol. 2019 Apr;75(4):570-578.
4. Van der Leest M, Israel B, Cornel EB, et al. High diagnostic performance of short magnetic resonance imaging protocols for prostate cancer detection in biopsy-naïve men: The Next Step in Magnetic Resonance Imaging Accessibility. Eur Urol 2019 Nov;76(5):574-581.