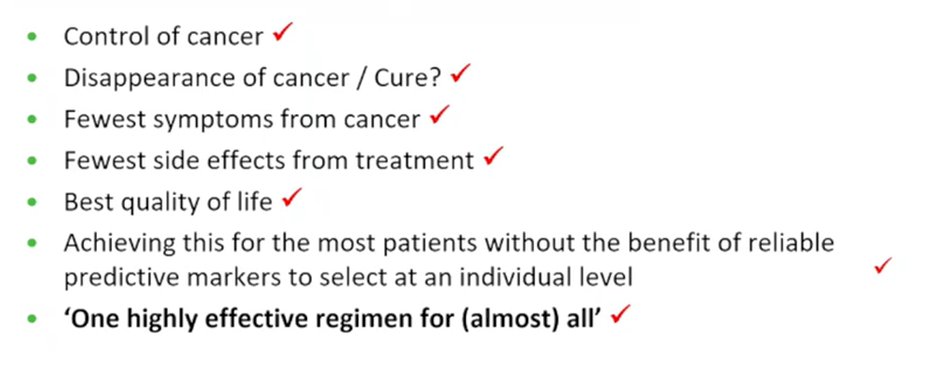
(UroToday.com) In the fifth session of the 2022 International Kidney Cancer Symposium (IKCS): Europe meeting focusing on first-line systemic therapy in advanced kidney cancer (metastatic renal cell carcinoma, mRCC), Dr. Pickering presented the first side of a debate regarding treatment selection, defending the approach of immune checkpoint inhibition combined with tyrosine kinase inhibitor (IO/TKI). In contextualizing this debate, she asked “what we want to achieve in first-line treatment of mRCC?”. She emphasized that we should be seeking to obtain the best outcomes for most patients. To this end, she highlighted “conventional endpoints” including control or shrinkage of cancer, the disappearance of cancer or cure, minimizing symptoms from cancer, minimizing side effects from treatment, and maximizing quality of life. These considerations must be premised on the basis of the fact that we do not have reliable predictive markers to select therapy at an individual level.
Dr. Pickering emphasized, in her only “biology” slide, that RCC is biologically diverse but strongly VEGF driven in the majority of patients. VEGF, highly expressed in renal tumors, promotes tumor growth via neoangiogenesis. Further, inhibiting VEGF leads to significant tumor regression. Thus, she suggested that, given a choice, we should want to target “the most ubiquitous” biological driver in RCC, rather than deliberately avoiding doing so.
She then discussed four relevant trials in this space, CheckMate-214, KEYNOTE-426, CLEAR, and CheckMate-9ER.
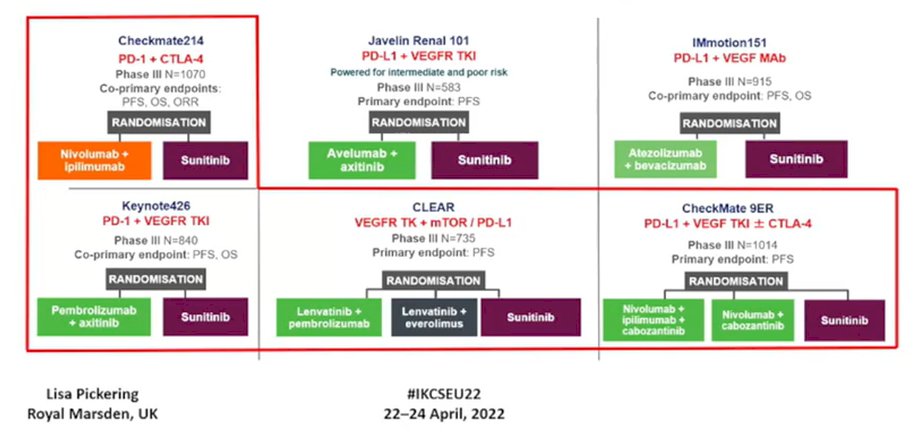
SharING a slide from Brian Rini that, with a caveat that formal comparisons across trials are fraught with issues, Dr. Pickering emphasized that there are differences between trials, particularly with respect to prognostic risk.
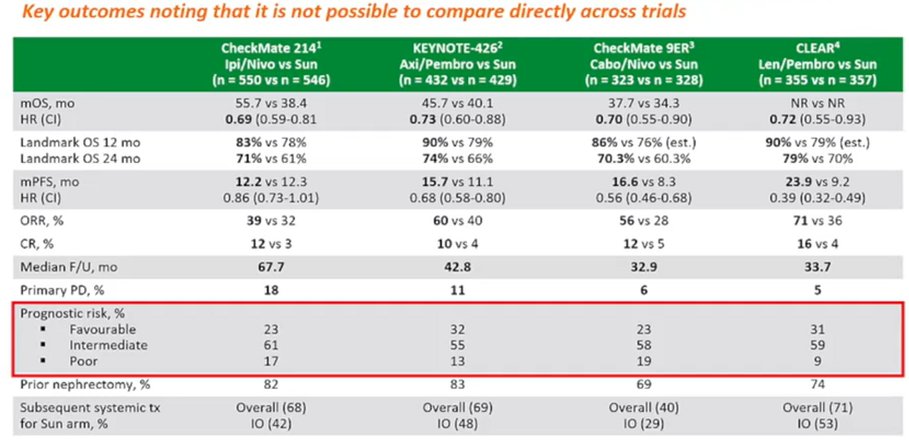
Overall, she emphasised that all of these treatment approaches are effective, with improved overall survival compared to sunitinib. Further, she emphasized that outcomes are “strikingly similar” across each of these treatment approaches. This is true whether we examine hazard ratios for death, as highlighted in the Kaplan Meier curves below, or landmark overall survival at 12 and 24 months.

In the context of these similarities, Dr. Pickering then emphasized differences between these treatment approaches. The first of these is the rapid onset of benefit in IO/TKI with early separation of the curves between a combined IO/TKI approach and sunitinib monotherapy. This splitting of the curve is seen both with respect to overall survival and with progression-free survival.

She emphasized that this may matter for some patients, particularly those in whom progression may affect quality of life. In contrast to these results from trials of the combination of IO/TKI, the separation of the curves occurs substantially slower in CheckMate-214 among patients who were treated with nivolumab and ipilimumab. Dr. Pickering highlighted an example of patients with chest wall disease who often have significant symptoms from their disease. Thus, these patients (along with others who may have significant symptoms or impending symptoms such as those with disease threatening major structures such as the brain, spine, pancreas, bone, or nodal disease) may benefit from more rapid treatment onset.
In terms of these quality of life effects, Dr. Pickering emphasized that response rate may be a more immediately meaningful endpoint than survival measure. Examining response rate, she emphasized that IO/IO has the lowest response rate and higher primary progressive disease. Therefore, TKI containing therapy is more likely to control symptoms and may be prioritized.

Dr. Pickering then moved to emphasize that an IO/TKI treatment approach is effective across all risk groups. In contrast, for those with favourable risk disease, nivolumab and ipilimumab have not shown benefit compared to sunitinib. She further considered the effect of toxicity and quality of life considerations on treatment selection. She commented that she had difficulty putting together a slide, in part due to heterogeneity between studies. She emphasized that toxicity and severe toxicity are typically manageable and rarely influence her treatment choices. However, the initial use of an IO/TKI approach gives more options for treatment modification which may be meaningful to manage treatment-related toxicity.
She highlighted that all cross-trial comparisons have meaningful limitations – however, these are intuitively difficult to avoid and the data for the combination IO/TKI approach are impressive in isolation. Further, she suggested that concerns regarding exhausting subsequent lines of therapy should not play into first-line treatment choice as we should focused on identifying the most effective regime for the current situation, rather than “saving” treatments for later. Finally, she addressed the question of a “long tail” on the curve for dual immune checkpoint inhibition, emphasizing that data suggest deep and long-lasting responses to approaches such as Lenvatinib/pembrolizumab and axitinib/pembrolizumab, though longer follow-up of these trials is needed. While there is longer follow-up from CheckMate-214, she suggested that comparisons between trials do not demonstrate meaningful differences in the tails of overall survival curves at comparable time points.
Thus, in conclusion, Dr. Pickering emphasized that an IO/TKI approach is a broadly efficacious treatment regime with a rapid treatment onset and durable and deep responses which is suitable for all patients, regardless of risk or subtype.
Presented by: Lisa Pickering, MD, PhD, Consultant Medical Oncologist, The Royal Marsden