(UroToday.com) The 2023 European Association of Urology (EAU) annual congress held in Milan, Italy between March 10th and 13th, 2023 was host to a plenary session addressing the “right management” of prostate cancer patients in the early detection and active surveillance settings.
Dr. Freddie Hamdy presented the updated 15-year oncologic outcomes of the PROstate TEsting for Cancer and Treatment (ProtecT) trial, which were concurrently published in The New England Journal of Medicine on the midnight of this EAU presentation.1
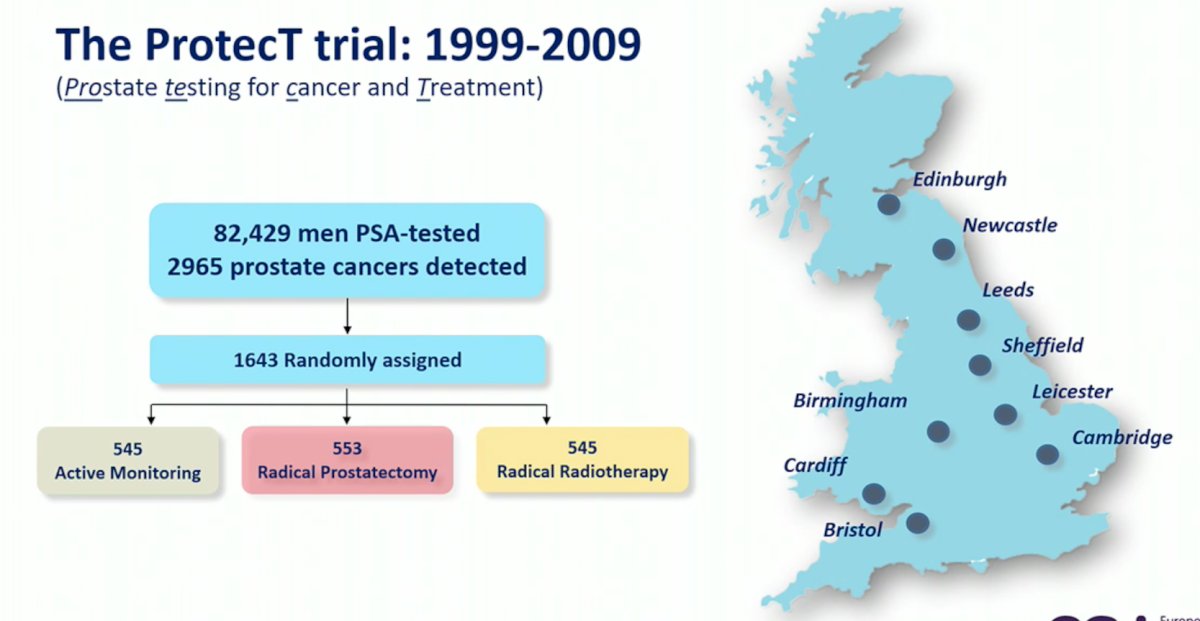
The PROstate TEsting for Cancer and Treatment (ProtecT) trial evaluated 82,429 men who underwent PSA testing between 1999 and 2009. Of these, 82,429 screened men, 2,965 were diagnosed with prostate cancer, of whom 1,643 were randomly assigned to:
- Active monitoring: 545
- Radical prostatectomy: 553
- Radical radiotherapy: 545
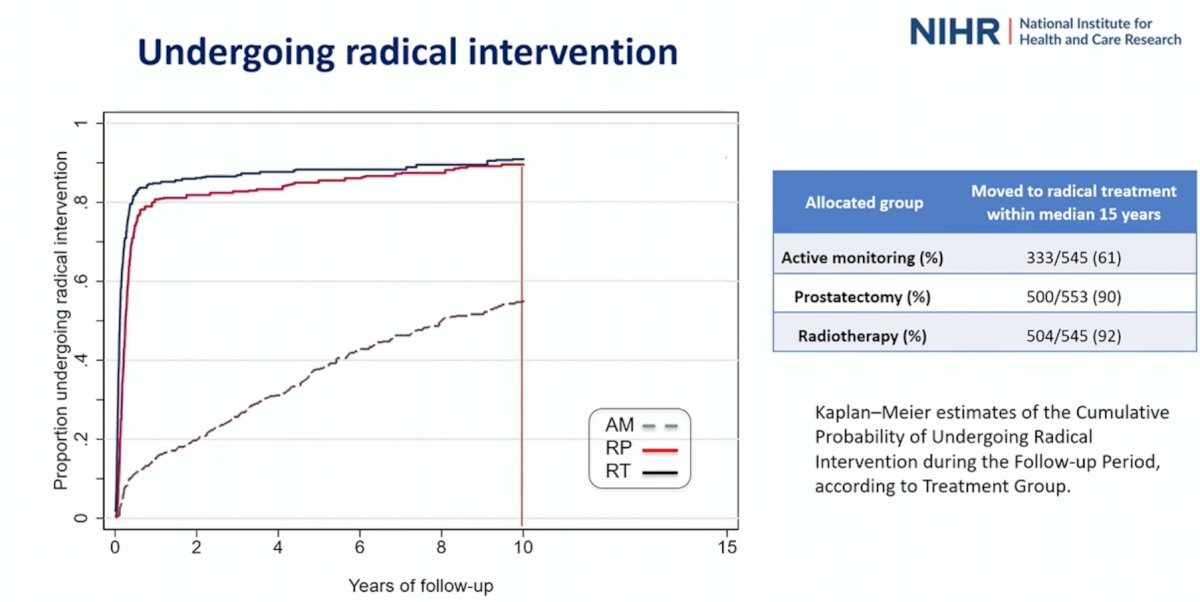
In this updated report, the percentage of patients undergoing radical intervention in the active monitoring group continued to increase, with 61% of patients initially randomized to active monitoring undergoing radical treatment within a median of 15 years. Conversely, 90% and 92% of patients in the prostatectomy and radiotherapy received radical therapy within the same time frame.
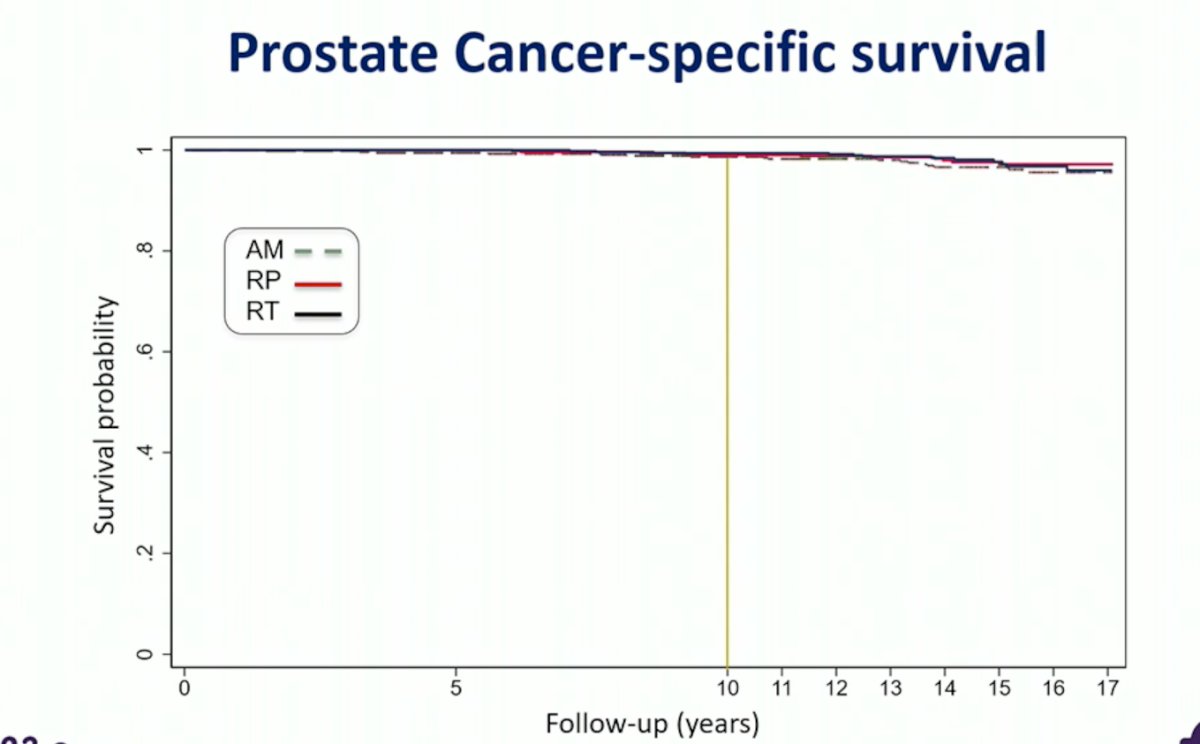
Similar to the findings from the 10-year report, prostate cancer-specific survival remained equally impressive across the three arms:
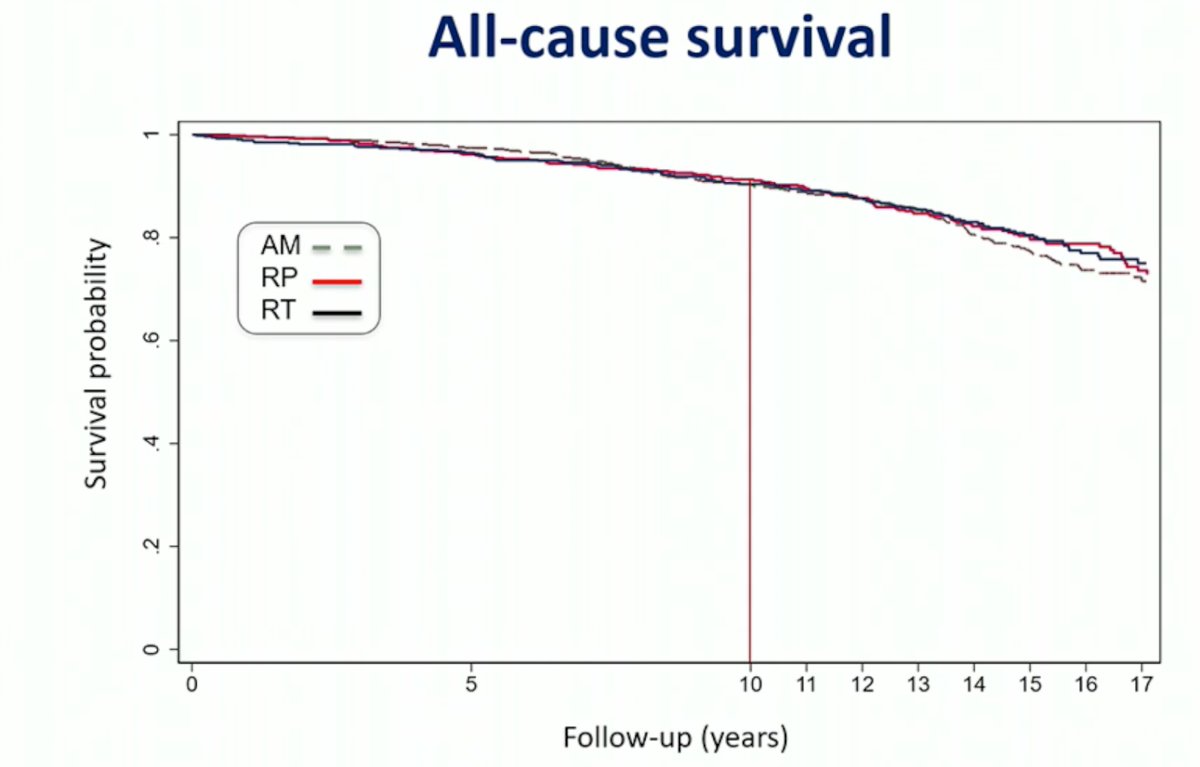
There were similarly no differences in all-cause survival between the three arms:
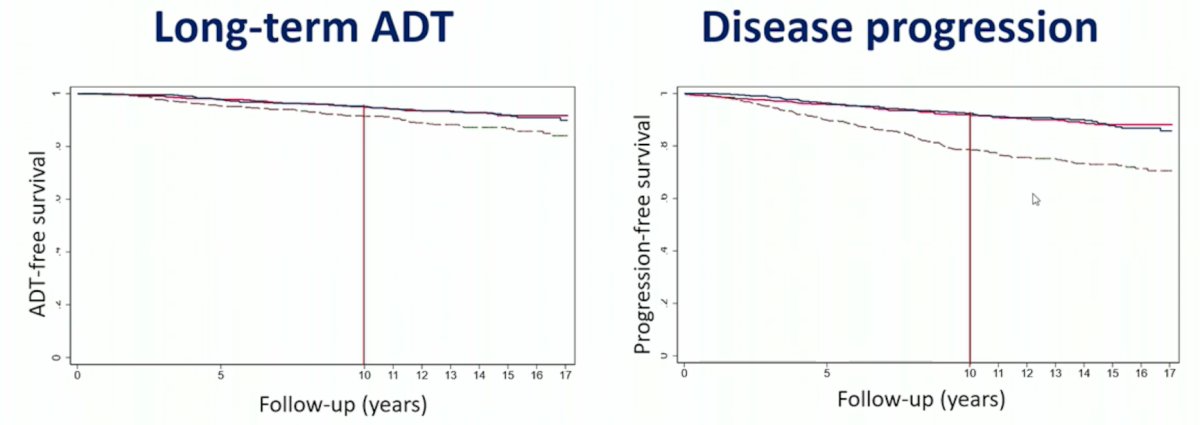
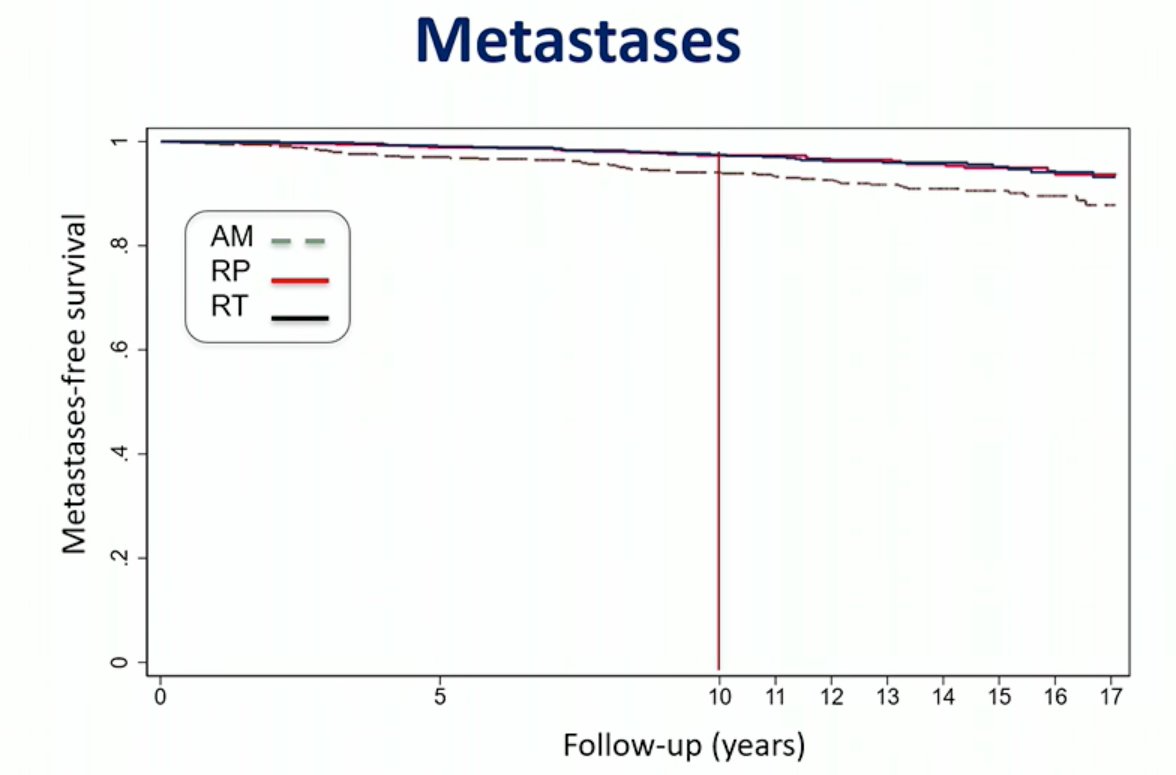
While the incidence of metastases, long-term ADT use, and disease progression rates were all significantly worse in the active monitoring group, these outcomes did not correspond to worse prostate cancer survival outcomes as previously seen in the above figures:
Dr. Hamdi next addressed common misconceptions pertaining to the ProtecT trial:
- ProtecT is not “just” a low-risk cohort of men with prostate cancer
- 34% were classified as intermediate risk using contemporary risk stratification
- One-third of ProtecT men receiving radical prostatectomy within 12 months of diagnosis had pT3 prostate cancer
- ProtecT is not disputing the need for aggressive treatment in high-risk prostate cancer
- Active monitoring as used in ProtecT is not “outdated”
- Despite its lower intensity compared to contemporary active surveillance, cancer-specific survival showed no difference compared with radical treatments
- “Modern technologies and innovations” such as mpMRI, PSMA-PET/CT, genetic testing, and other biomarkers are reportedly reliable in the post-diagnostic space to decide on treatments
- Where is the evidence that outcomes and cancer-specific survival outcomes improve?
As demonstrated in the table below, 34% of men had D’Amico intermediate or high-risk disease.

A deeper analysis of the patients who had a radical prostatectomy and died of prostate cancer, demonstrated that 100% were upstaged and 77% upgraded at time of surgery:

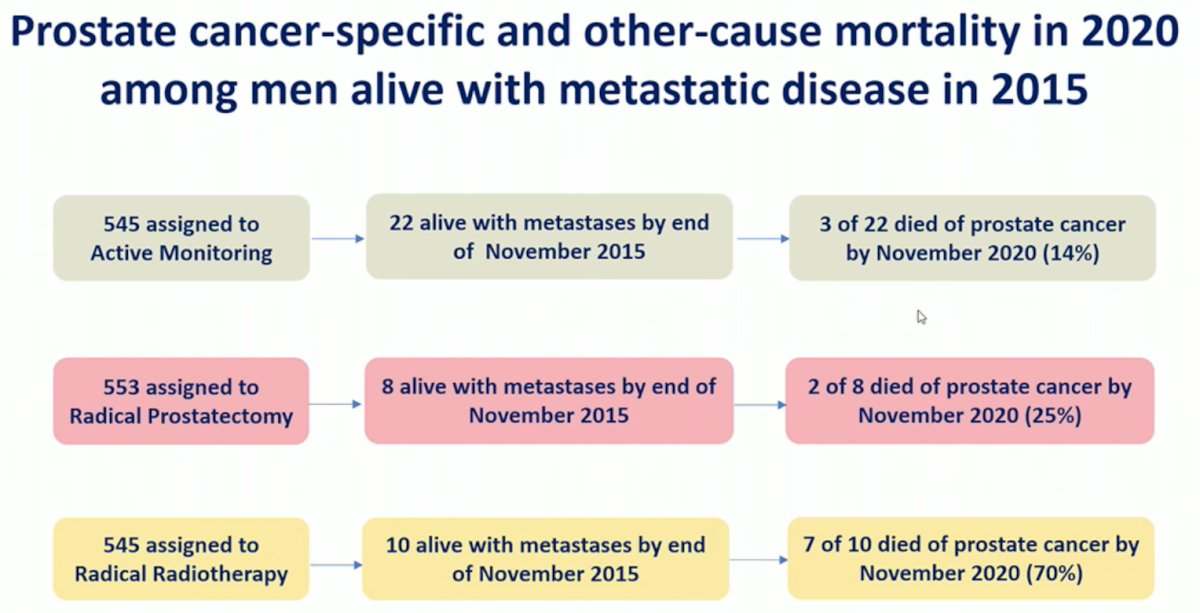
While the incidence of metastases was higher in the active monitoring group, this did not correspond to worse cancer survival outcomes. As such, in this updated report, Dr. Hamdy and colleagues evaluated survival outcomes in patients who developed metastases, by randomization group:
Dr. Hamdy concluded his presentation of the 15-year outcomes with the following key messages:
- Survival from clinically localized prostate cancer remains very high over a median of 15 years (96-97%), irrespective of treatment allocation
- Men with metastases do not necessarily die of prostate cancer
- Men who die of prostate cancer have lethality features, yet to be identifiable and are not easily impacted by multimodality treatment approaches
- Current risk-stratification methods are unreliable and new tools are needed
- The indications for active monitoring/surveillance can be safely expanded to intermediate-risk disease
- The long survival of screen-detected prostate cancer men in ProtecT with or without treatment, with or without metastases does not support the introduction of population testing for early detection
- Treatment decisions need to balance “trade-offs” between the reduction of metastases, long-term hormones, and local progression with radical treatments against their short-, medium-, and long-term impacts on sexual, urinary, and bowel function
Presented by: Freddie Hamdy, MD, FRCS(Urol), FMedSci, Nuffield Professor of Surgery and Urology at the University of Oxford, Oxford, England
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 European Association of Urology (EAU) Annual Meeting, Milan, IT, Fri, Mar 10 – Mon, Mar 13, 2023.
Reference:Related Content: EAU 2023: 15-year update ProtecT trial - Part II: Quality of Life