(UroToday.com) The 2022 EAU annual meeting featured a joint session of the EAU, EANM, ESMO, and ESTRO societies examining modern diagnostic and therapeutic approaches in prostate cancer, including a presentation by Dr. Gert De Meerleer discussing radiotherapy as a salvage treatment option for the PSMA avid lesion in the setting of recurrent prostate cancer. Dr. De Meerleer started by discussing the very recently published study from Zamboglou et al.,1 which examined (i) metastasis-free survival (MFS) following PSMA-PET guided salvage radiotherapy and (ii) the metastatic patterns on PSMA-PET images after salvage radiotherapy. This retrospective, multicenter (9 centers, 5 countries) study included 815 patients referred for PSMA-PET due to recurrent/persistent disease after prostatectomy. All patients received intensity-modulated radiotherapy to the prostatic fossa, and in case of PET-positive pelvic lymph nodes (n=275, 34%), pelvic lymphatics had been irradiated. Additionally, ADT had been previously given in 251 (31%) patients. The median follow-up after salvage radiotherapy was 36 months, and the 2-year MFS rate was 93% and 4-year rate following salvage radiotherapy was 81%. On multivariate analysis, the presence of PET-positive pelvic lymph nodes was a strong predictor for MFS (HR=2.39, p<0.001):

Following salvage radiotherapy, distant metastasis was detected by PSMA-PET in 128/198 (65%) patients and two metastatic patterns were observed: 43% had distant metastasis in sub diaphragmatic para-aortic lymph nodes (abdominal-lymphatic) whereas 45% in bones, 9% in supra diaphragmatic lymph nodes and 6% in visceral organs (distant). The Kaplan-Meier curve for MFS stratified by PET-negative lymph nodes and PET-positive lymph nodes is as follows:

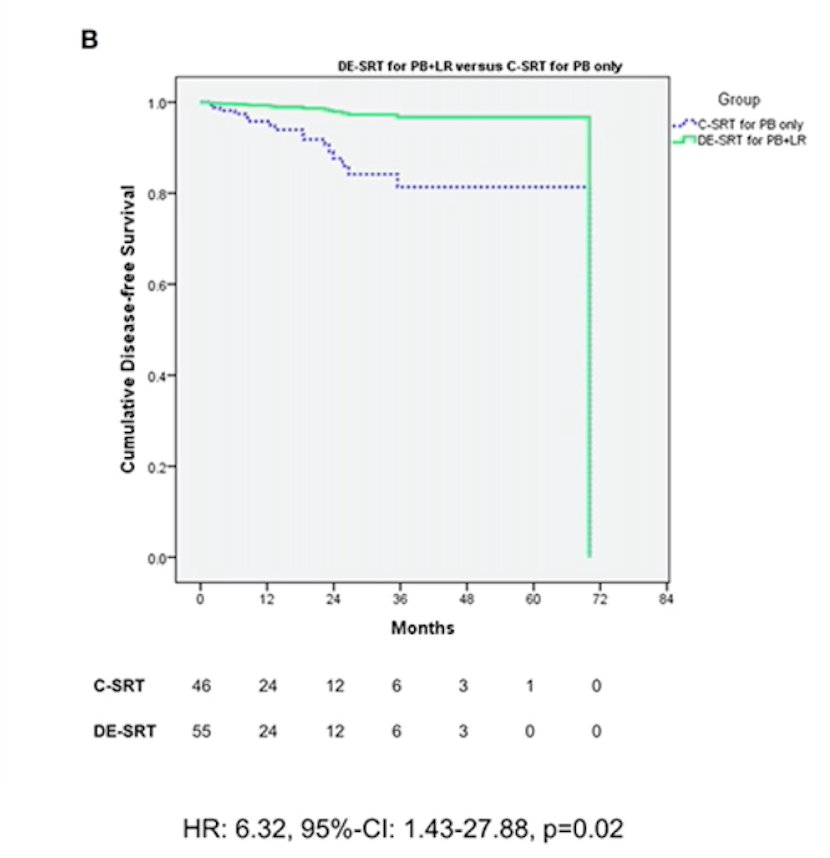
Dr. De Meerleer notes that the SAKK 09/10 trial aimed to compare conventional and dose-intensified salvage radiotherapy, randomizing patients to conventional-dose (64 Gy) or dose-intensified salvage radiotherapy (70 Gy) to the prostate bed without hormonal therapy.2 After median follow-up of 6.2 years, the median freedom from biochemical recurrence was 8.2 years in the 64 Gy arm and 7.6 in the 70 Gy arm (log-rank p = 0.4), with a hazard ratio of 1.14 (95% CI 0.82-1.60). Vogel et al.3 have also assessed the feasibility and outcomes of PSMA PET-based dose-escalated salvage radiotherapy versus conventional salvage radiotherapy for patients with recurrent prostate cancer. This study evaluated 199 patients who were treated with salvage radiotherapy, including 101 patients who received dose-escalated salvage radiotherapy with simultaneous integrated boost for PET-positive local recurrence and/or PET-positive lymph nodes, and 98 patients were treated with conventional salvage radiotherapy to the prostate bed +/- elective pelvic lymphatic pathways without simultaneous-integrated boost. All patients received PSMA-PET imaging prior to dose-escalated salvage radiotherapy (68Ga-PSMA-11: 45.5%; 18F-labeled PSMA: 54.5%). Cumulative disease-free survival favored the dose-escalated salvage radiotherapy group (HR 6.32, 95% CI 1.43-27.88), with no difference in acute and late toxicity grade 3 adverse events:
Dr. De Meerleer cautions that salvage radiotherapy should be postponed until a PSMA PET-positive result is observed. In a study by Schiller et al.,4 among 233 patients receiving 68Ga-PSMA-PET/CT with 799 lymph node metastases, it was noted that the vast majority of lymph nodes not covered in the RTOG clinical target volume are situated in the para-aortal, pararectal, paravesical, preacetabular, presacral, and inguinal regions:

PSA levels at the time of PET/CT imaging had the highest predictive value for extrapelvic metastatic lymph node spread, such that for every increase of 1 ng/mL in PSA raises the risk of metastases outside the clinical target volume by a factor of 1.43. As such, Dr. De Meerleer cautions that it is imperative that urologists do not wait for the PSA to get above 0.20 ng/mL before referring to radiation oncology in order to not miss the window for cure.
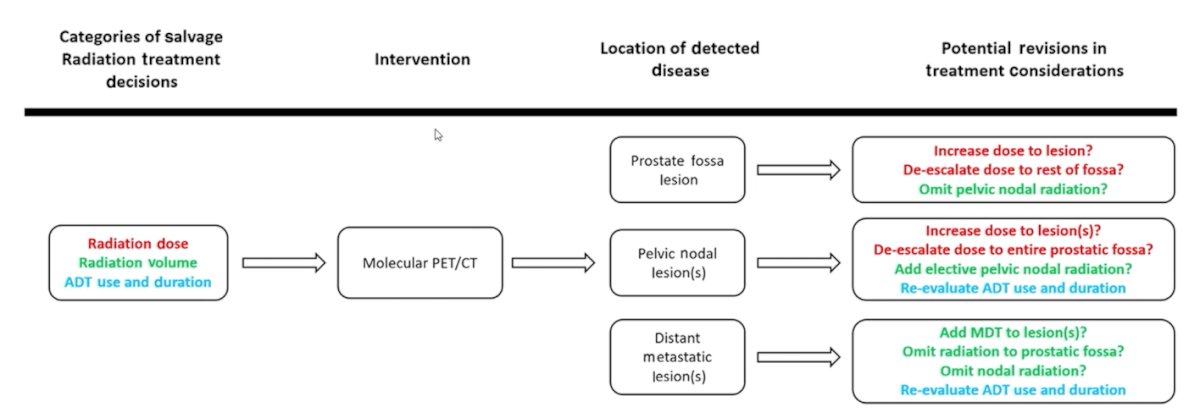
Dr. De Meerleer concluded his presentation discussing radiotherapy as a salvage treatment option for the PSMA avid lesion in the setting of recurrent prostate cancer with the following take-home message figure:
Presented By: Gert De Meerleer, MD, PhD, Department of Radiation Oncology, University Hospitals Leuven, Leuven, Belgium
Written By: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 European Association of Urology (EAU) Annual Hybrid Meeting, Amsterdam, NL, Fri, July 1 – Mon, July 4, 2022.
References:
- Zamboglou C, Strouthos I, Sahlmann J, et al. Metastasis-free survival and patterns of distant metastatic disease after PSMA-PET-guided salvage radiotherapy in recurrent or persistent prostate cancer after prostatectomy. Int J Radiat Oncol Biol Phys. 2022 Jun 2;S0360-3016(22)00409-6.
- Ghadjar P, Hayoz S, Bernhard J, et al. Dose-intensified versus conventional-dose salvage radiotherapy for biochemically recurrent prostate cancer after prostatectomy: The SAKK 09/10 Randomized Phase 3 Trial. Eur Urol. 2021 Sep;80(3):306-315.
- Vogel MME, Dewes S, Sage EK, et al. Feasibility and outcome of PSMA-PET-based dose-escalated salvage radiotherapy versus conventional salvage radiotherapy for patients with recurrent prostate cancer. Front Oncol. 2021;11:715020.
- Schiller K, Stohrer L, Dusberg M, et al. PSMA-PET/CT-based lymph node atlas for prostate cancer patients recurring after primary treatment: clinical implications for salvage radiation therapy. Eur Urol Oncol. 2021 Feb;4(1):73-83.