For this purpose, the authors carried out a retrospective multicenter analysis of patients with RCC who underwent surgical treatment between 2006 and 2017. All patients were divided into two groups, depending on whether the pre-treatment CRP level was normal (≤0.5mg/L) or elevated CRP (>0.5mg/L). Multivariable analyses (MVA) and Kaplan-Meier Analyses (KMA) were utilized to delineate freedom from and predictors for eGFR<60, <45, and <30.
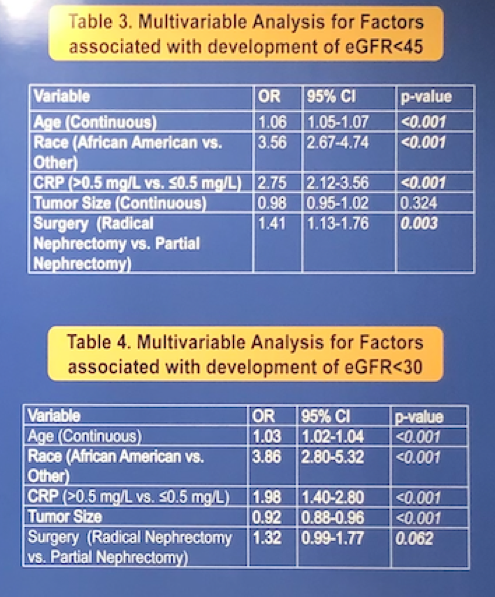
A total of 2,693 patients who underwent radical (RN) or partial nephrectomy (PN) were analyzed. From these, 1,198 patients had a normal-CRP level, while in 1,495 cases it was elevated. Median follow-up was 22 months. Elevated-CRP patients were more frequently African-American (20.9% vs. 2.8%, p<0.001) with larger median tumor size (6.1 cm vs. 4.0 cm, p<0.001). According to MVA, elevated-CRP was independently associated with development of de novo eGFR<60 (OR=2.56, p<0.001), eGFR<45 (OR=2.75, p<0.001), and eGFR<30 (OR=1.98, p<0.001). KMA revealed significantly higher 5-year freedom from de novo eGFR<45 for normal-CRP as opposed to elevated-CRP (68.5% vs. 43.5%, log-rank p<0.001).
Authors concluded that pre-treatment elevated CRP had been independently associated with progressive renal functional decline in patients with RCC undergoing surgery. Based on the study results, a close functional follow up and renoprotective strategies are required for patients with elevated CRP at baseline as well as a strong attempt to perform nephron-sparing surgery when feasible and appropriate. During the discussion, two important considerations were highlighted. First of all, an elevated CRP level can be associated with the secretion by the tumor itself. But as prof. Derweesh pointed out, in those cases with persisted elevation of CRP after surgery, it is necessary to close follow-up the patients with involvement of nephrologist. The second point is a non-specific nature of CRP which can be influenced by multiple factors, such as inflammation or infectious process. However, the CRP level is a cheap and readily available test. Finally, this team of authors presented another study dedicated to the evaluation of a novel scoring index CART (C-reactive protein, age, race, tumor size) for prediction of renal functional decline post partial nephrectomy. Therefore, an exact role of elevated CRP level in this cohort of patients deserves further study.
Presented by: Ithaar H. Derweesh, MD, Urologic Oncologist, Professor of Urology and Radiology, the University of California San Diego, Department of Urology, San Diego, United States.
Written by: Kirill Shiranov, MD, Fellow, Department of Urology, Rostov University, Rostov on Don, Russia, Twitter: @endourologist and Zhamshid Okhunov, MD, Twitter: @OkhunovZham, Department of Urology, University of California-Irvine at the 34th European Association of Urology (EAU 2019) #EAU19, conference in Barcelona, Spain, March 15-19, 2019.