(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to the "Common Problems and Controversies in Bladder Cancer: Rapid-Fire Debates" session, developed and led by Dr. Ashish Kamat. Following a case presentation by Dr. Benjamin Pradere, Dr. Fernando Maluf argued that bladder preservation in muscle-invasive bladder cancer (MIBC) patients with a clinical complete response (cCR) is a smart, data-driven strategy, whereas Dr. Bogdana Schmidt argued that bladder preservation in these patients remains ‘risky business’.
Dr. Pradere presented a case of an 80-year-old male with an excellent performance status, past medical history of hypertension, and a 20-pack-year smoking history who presented with gross hematuria. He was found to have an aggressive appearing papillary tumor on cystoscopy, and a subsequent transurethral resection of bladder tumor (TURBT) demonstrated:
- Urothelial carcinoma 95%; micropapillary variant 5%
- cT2
- CIS +ve
- Lymphovascular invasion (LVI) +ve
He was planned for neoadjuvant chemotherapy (NAC) followed by a radical cystectomy and received six cycles of dose dense MVAC (ddMVAC). Following completion of NAC, the patients asked: “Can we avoid a cystectomy?”.
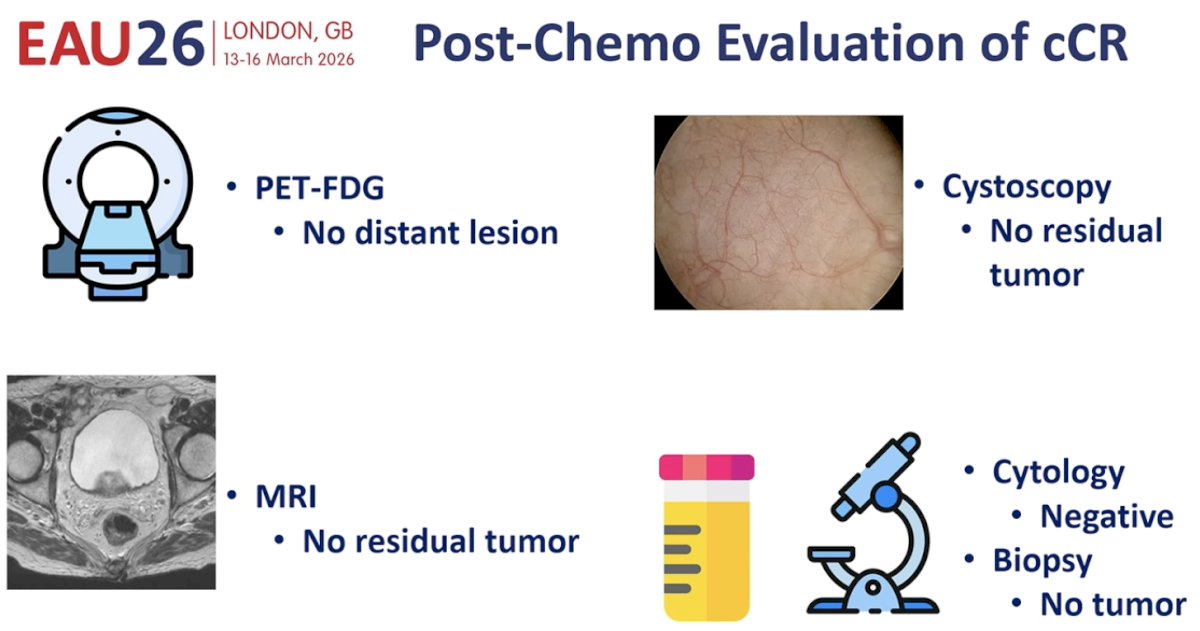
The patient underwent a thorough evaluation as follows:
- FDG-PET: No distant disease
- MRI: No residual tumor
- Cystoscopy + biopsy: No residual tumor
- Urine cytology: Negative
Is bladder preservation reasonable in this setting?
Dr. Maluf argued that bladder preservation is a smart, data-driven strategy and reasonable for this patient. He emphasized that bladder preservation should be considered within a modern framework of precision oncology. He proposed that a “smart-driven strategy for organ preservation” relies on integrating pathology, imaging, mutation analysis, circulating tumor DNA (ctDNA), and urinary tumor DNA (utDNA) to identify patients who have achieved a true pathologic complete response (pCR).
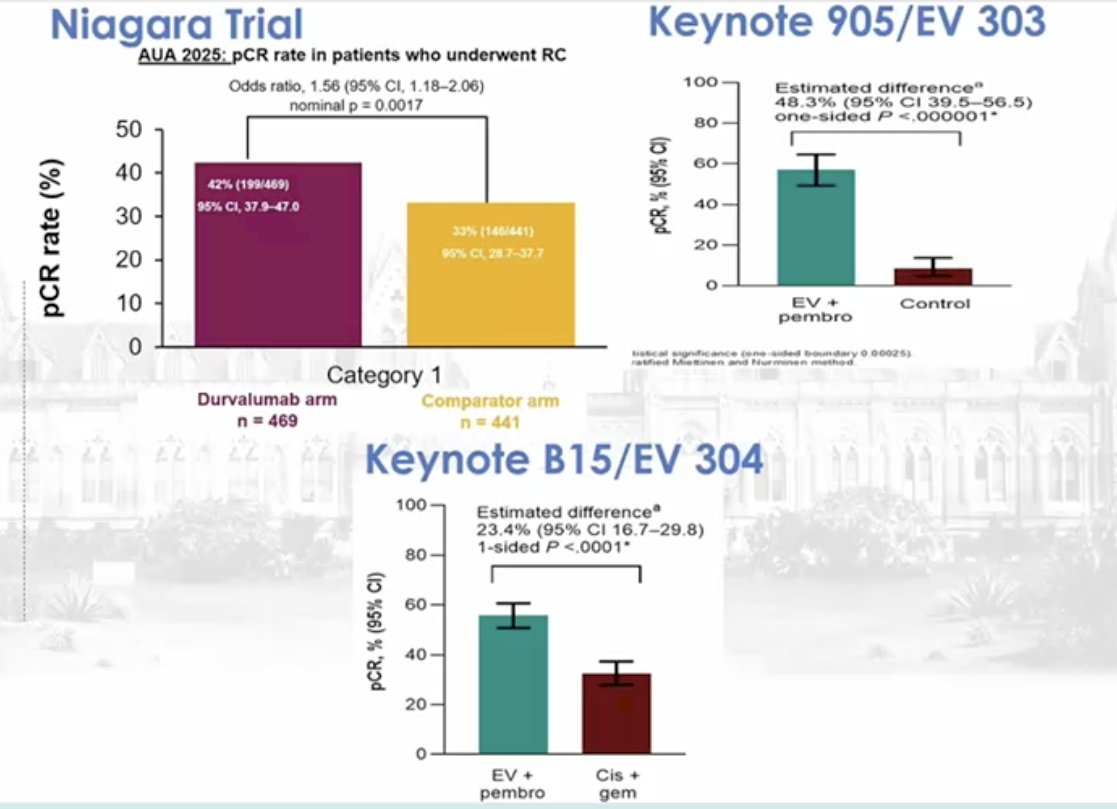
He first highlighted improvements in pCR rates achieved with modern systemic therapies. Data from the phase III NIAGARA trial evaluating perioperative durvalumab with cisplatin-based chemotherapy demonstrated an improvement in pCR rates, whereby the durvalumab-containing arm achieved a pCR of 42% compared with 35% in the comparator arm, corresponding to an odds ratio of 1.56 (95% CI 1.18–2.06; nominal p=0.0017).1 Similarly, the KEYNOTE 905/EV-303 trial of perioperative enfortumab vedotin plus pembrolizumab (EV+P) in cisplatin-ineligible patients demonstrated a pCR of 58.3% with EV+P.2 The corresponding proportion in the KEYNOTE B15/EV-304 trial in cisplatin-eligible patients demonstrated a pCR of 55% with EV+P versus 32% with cisplatin combination chemotherapy.3
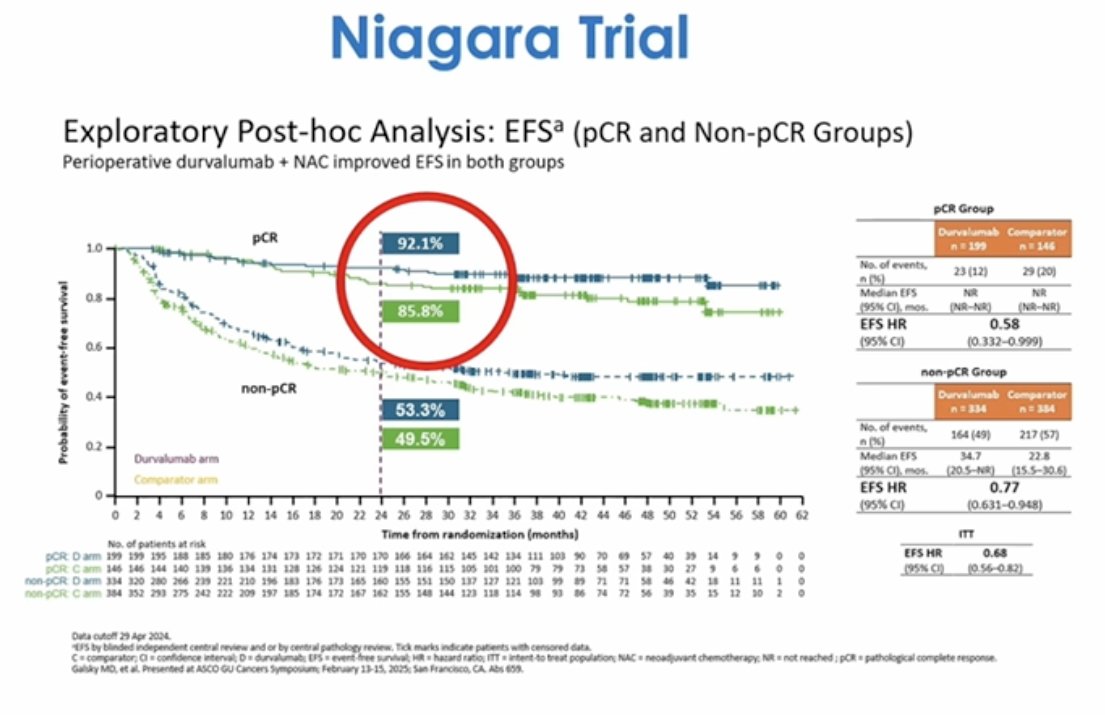
Importantly, exploratory analyses from NIAGARA evaluating event-free survival (EFS) according to pathologic response demonstrated the strong prognostic significance of a complete response. In patients achieving pCR, EFS was approximately 92.1% in the durvalumab arm compared with 85.8% in the comparator group. In contrast, among patients without pCR, event-free survival was substantially lower, approximately 53.3% versus 49.5%. These findings underscore that achieving a complete response identifies a group of patients with excellent long-term outcomes, facilitating potential bladder-sparing approaches.
Dr. Maluf next highlighted data supporting response-adapted organ preservation from the phase II trial evaluating gemcitabine, cisplatin, and nivolumab as an organ-sparing strategy for muscle-invasive bladder cancer.4 This study provides an important framework for understanding how clinical complete response (cCR) after systemic therapy may translate into favorable long-term outcomes and potentially allow safe avoidance of radical cystectomy in selected patients.
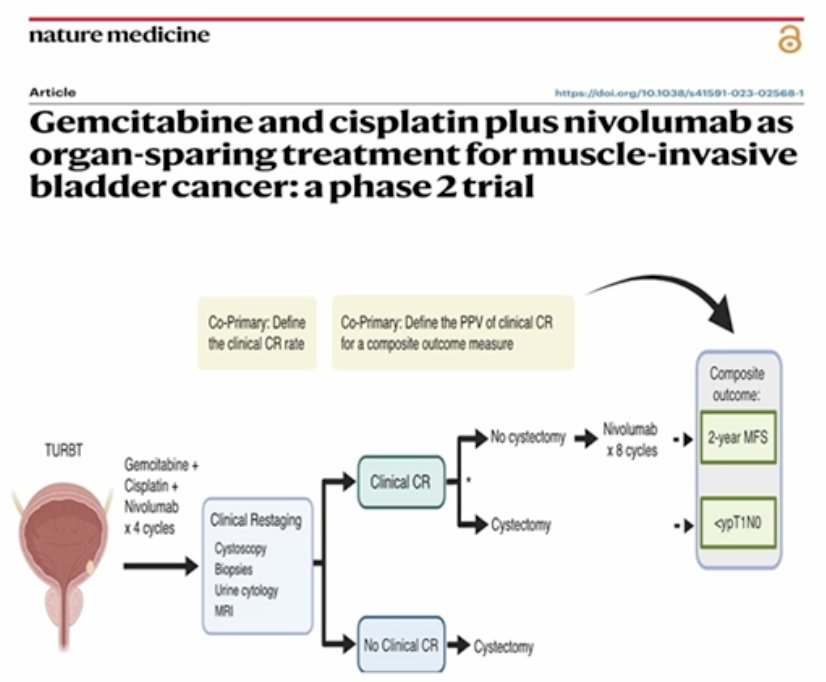
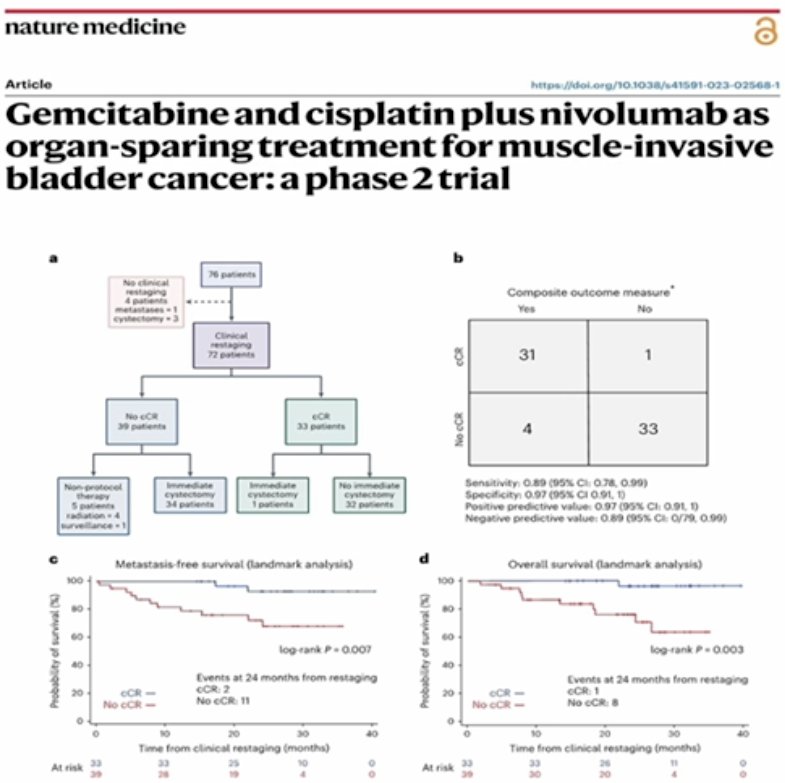
The study enrolled 76 patients treated with ‘neoadjuvant’ gemcitabine, cisplatin, and nivolumab x 4 cycles. Four patients did not undergo clinical restaging, including one patient who developed metastatic disease and three patients who proceeded directly to cystectomy, leaving 72 patients evaluable for response assessment. Among these 72 patients, 33 (46%) achieved a clinical complete response, and 39 (54%) did not.
Management decisions following restaging reflected the response status. Among the 39 patients without a cCR, the majority proceeded directly to immediate cystectomy (34 patients), while a small number received non-protocol therapy or radiation or were observed. In contrast, among the 33 patients with a cCR, only one patient underwent immediate cystectomy, while 32 patients avoided immediate surgery, effectively demonstrating the feasibility of an organ-preserving strategy in this population.
Importantly, the investigators evaluated how accurately cCR predicted a favorable oncologic outcome. The contingency table demonstrated a very strong association between clinical response and a composite outcome measure. Thirty-one patients with cCR achieved the composite endpoint compared with only one patient with cCR who did not. Conversely, among patients without a cCR, 33 failed to achieve the composite outcome while only four achieved it. These findings translated into a sensitivity of 0.89 (95% CI 0.78–0.99) and a specificity of 0.97 (95% CI 0.91–1.0), with a positive predictive value of 0.97 and a negative predictive value of 0.89. This high predictive accuracy supports the concept that carefully defined clinical complete response may serve as a reliable surrogate for favorable oncologic outcomes.
Dr. Maluf emphasized that the most compelling data from this study come from the landmark survival analyses beginning at the time of clinical restaging. Patients achieving a cCR demonstrated markedly superior metastasis-free survival compared with those without. At 24 months following restaging, only two metastatic events were observed in the clinical complete response group compared with eleven events among patients without clinical complete response (p=0.007). These findings demonstrate that achieving cCR identifies a population with substantially lower risk of metastatic progression.
A similar pattern was observed for overall survival. Again, using a landmark approach beginning at clinical restaging, patients with cCR demonstrated excellent long-term survival compared with those without a clinical complete response. At 24 months, only one death occurred among patients with clinical complete response compared with eight deaths in the non-CCR group (p=0.003). Taken together, these survival analyses strongly suggest that cCR following chemoimmunotherapy identifies a group of patients with particularly favorable biology and excellent outcomes.
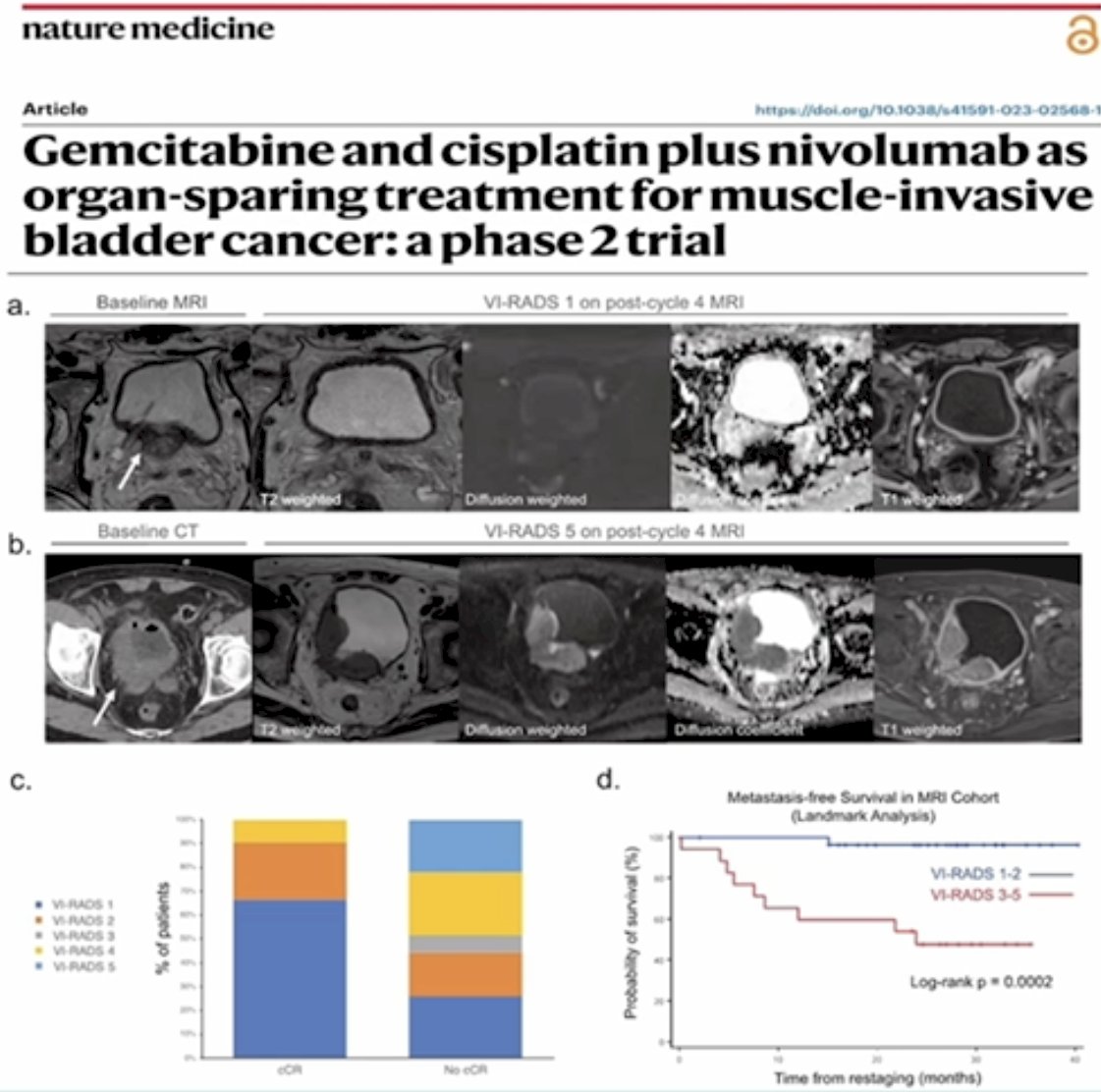
Imaging has also emerged as an important tool for identifying residual disease following neoadjuvant therapy. Multiparametric MRI using the Vesical Imaging Reporting and Data System (VI-RADS) can stratify patients according to the likelihood of residual tumor. In the analysis presented, patients with VI-RADS scores of 1–2 after chemotherapy demonstrated excellent metastasis-free survival, whereas patients with VI-RADS scores of 3–5 experienced significantly worse outcomes (p=0.002; figure below). These findings suggest that imaging may provide a non-invasive method for identifying patients with a high probability of complete response.
Dr. Maluf next transitioned from imaging-based response assessment to emerging molecular biomarkers that may refine patient selection for bladder preservation strategies. He highlighted that ctDNA and utDNA are increasingly being investigated as tools to identify patients who achieve true pCR following neoadjuvant therapy.
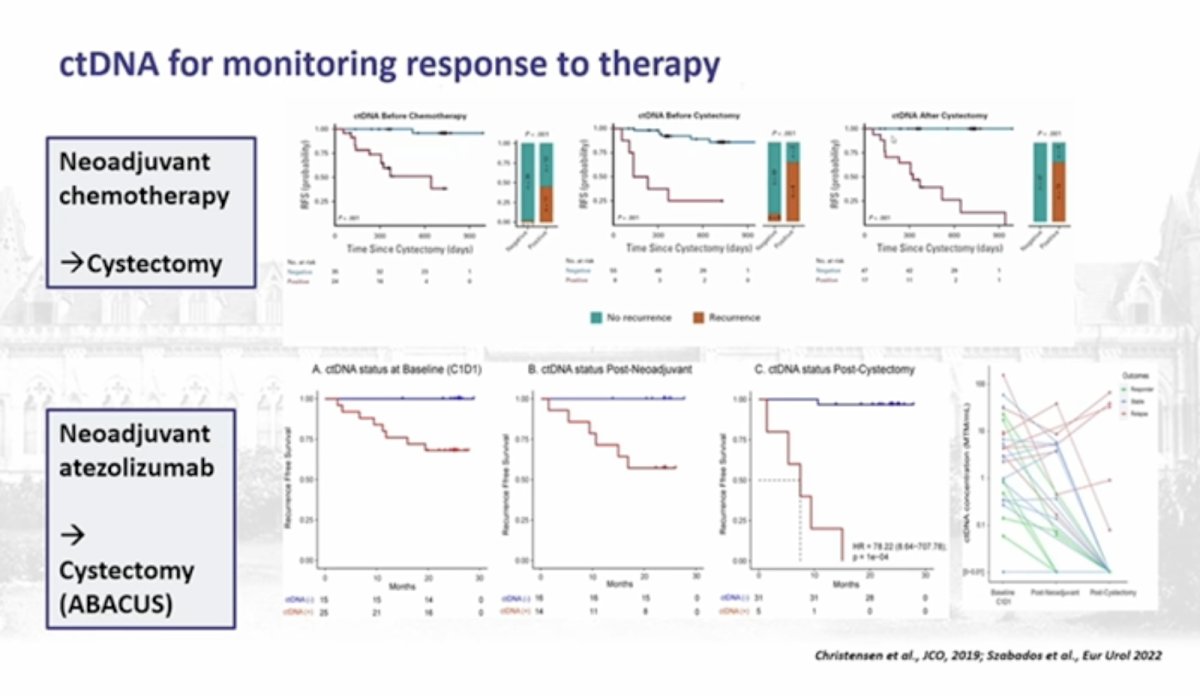
He first highlighted the role of ctDNA for monitoring treatment response in MIBC. Data from cohorts of patients receiving NAC followed by cystectomy demonstrate that ctDNA status is strongly associated with oncologic outcomes. Patients with detectable ctDNA prior to cystectomy exhibit significantly worse recurrence-free survival compared to those who are ctDNA negative. Kaplan–Meier analyses in these cohorts show clear separation of survival curves, with ctDNA-positive patients experiencing markedly higher recurrence rates after cystectomy. Conversely, ctDNA clearance following neoadjuvant therapy correlates with improved outcomes, suggesting that ctDNA may function as a dynamic biomarker of minimal residual disease. These findings are supported by translational analyses demonstrating that ctDNA positivity after neoadjuvant therapy predicts early systemic relapse.
Dr. Maluf then referenced results from the ABACUS study, which evaluated neoadjuvant atezolizumab prior to cystectomy in patients with muscle-invasive bladder cancer.5 In this dataset, ctDNA status was evaluated longitudinally at baseline, following neoadjuvant therapy, and after cystectomy. Kaplan–Meier analyses again demonstrated a clear prognostic signal. Patients who were ctDNA negative following neoadjuvant immunotherapy experienced substantially improved recurrence-free survival compared to ctDNA-positive patients, supporting the concept that ctDNA may identify patients with eradicated systemic disease.
He next discussed prospective data from the RETAIN-2 study,6 which integrated molecular biomarkers into treatment decision-making after neoadjuvant therapy. RETAIN-2 enrolled patients with cT2–T3N0 muscle-invasive bladder cancer who received neoadjuvant nivolumab combined with accelerated MVAC. Tumor sequencing was performed to identify mutations in DNA damage response genes, including ATM, RB1, and ERCC2. Patients demonstrating both mutation positivity and cCR were allowed to enter an active surveillance strategy rather than proceeding directly to radical cystectomy.
Outcomes from the active surveillance cohort provide important insight into the feasibility of bladder preservation in carefully selected patients. Among 22 patients managed with active surveillance, the majority remained recurrence-free during follow-up. However, local recurrence occurred in a subset of patients, highlighting that while systemic control may be achieved, intravesical relapse remains a significant concern. Importantly, all metastatic recurrences in this cohort were preceded by local recurrence events, suggesting that early detection of bladder relapse remains critical for maintaining oncologic safety in bladder preservation strategies.

Further analysis from RETAIN demonstrated that post-neoadjuvant ctDNA status may help stratify risk. Among 40 evaluated patients, ctDNA negativity following neoadjuvant therapy was associated with substantially improved metastasis-free survival compared to ctDNA positivity. Specifically, 82.6% of ctDNA patients remained metastasis-free, compared with 51.4% among ctDNA+ patients. These findings suggest that ctDNA may be particularly informative for predicting systemic relapse risk, although it appears less predictive for local recurrence within the bladder.
Dr. Maluf then shifted to emerging data on utDNA as an additional biomarker that may complement ctDNA analysis. He presented results from translational analyses within the NIAGARA trial, which evaluated perioperative durvalumab combined with chemotherapy in muscle-invasive bladder cancer. In these analyses, both utDNA and ctDNA were assessed prior to cystectomy to evaluate associations with pathologic response and residual disease burden.
Pre-cystectomy utDNA status demonstrated a strong correlation with pathologic complete response. Patients who were utDNA- prior to surgery exhibited significantly higher rates of pCR compared to utDNA+ patients. In contrast, utDNA positivity was associated with persistent residual disease at cystectomy. Additional analyses demonstrated that utDNA and ctDNA appear to reflect different biological processes. UTDNA positivity was associated with a higher likelihood of residual intravesical disease, consistent with the detection of tumor DNA shed locally within the bladder. By contrast, ctDNA positivity was associated with higher rates of nodal involvement and more advanced disease stage at cystectomy, suggesting that ctDNA reflects systemic tumor dissemination.
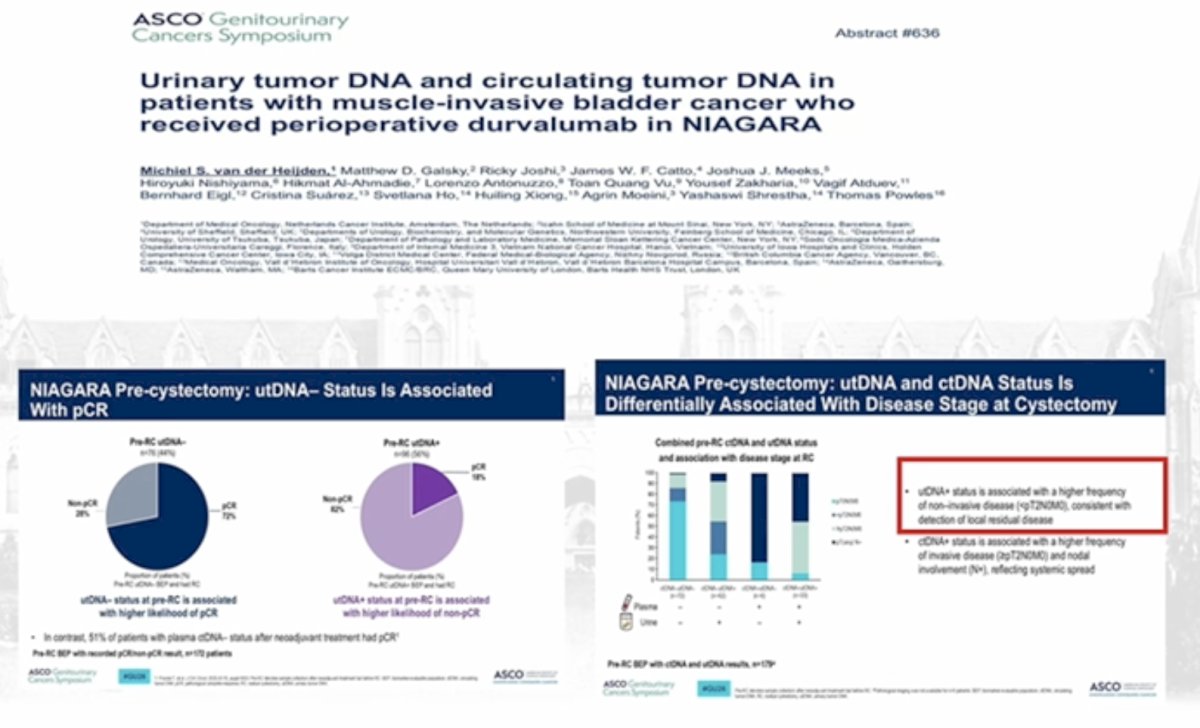
Taken together, these findings suggest that integrating ctDNA and utDNA may provide complementary information regarding residual disease biology following neoadjuvant therapy. utDNA may be particularly useful for detecting persistent bladder-confined disease, while ctDNA may identify patients at risk for systemic relapse.
Dr. Maluf then introduced the REDEMPTED trial, which aims to prospectively evaluate biomarker-driven bladder preservation strategies. In this study, MIBC patients will receive neoadjuvant cisplatin and gemcitabine combined with durvalumab for four cycles. Following neoadjuvant therapy, patients undergo maximal TURBT and restaging evaluation. Patients demonstrating favorable biomarker profiles may proceed to bladder preservation using chemoradiation, consisting of weekly cisplatin with radiotherapy for four weeks, followed by adjuvant durvalumab for eight cycles. Alternatively, patients may proceed to radical cystectomy with adjuvant durvalumab.
Importantly, ctDNA and utDNA are evaluated at multiple time points within this study, including (i) prior to neoadjuvant therapy, (ii) before local treatment, and (iii) following chemoradiation in the bladder preservation arm. The primary endpoint of the trial is metastasis-free survival, with the goal of determining whether molecular biomarkers can reliably identify patients suitable for bladder preservation.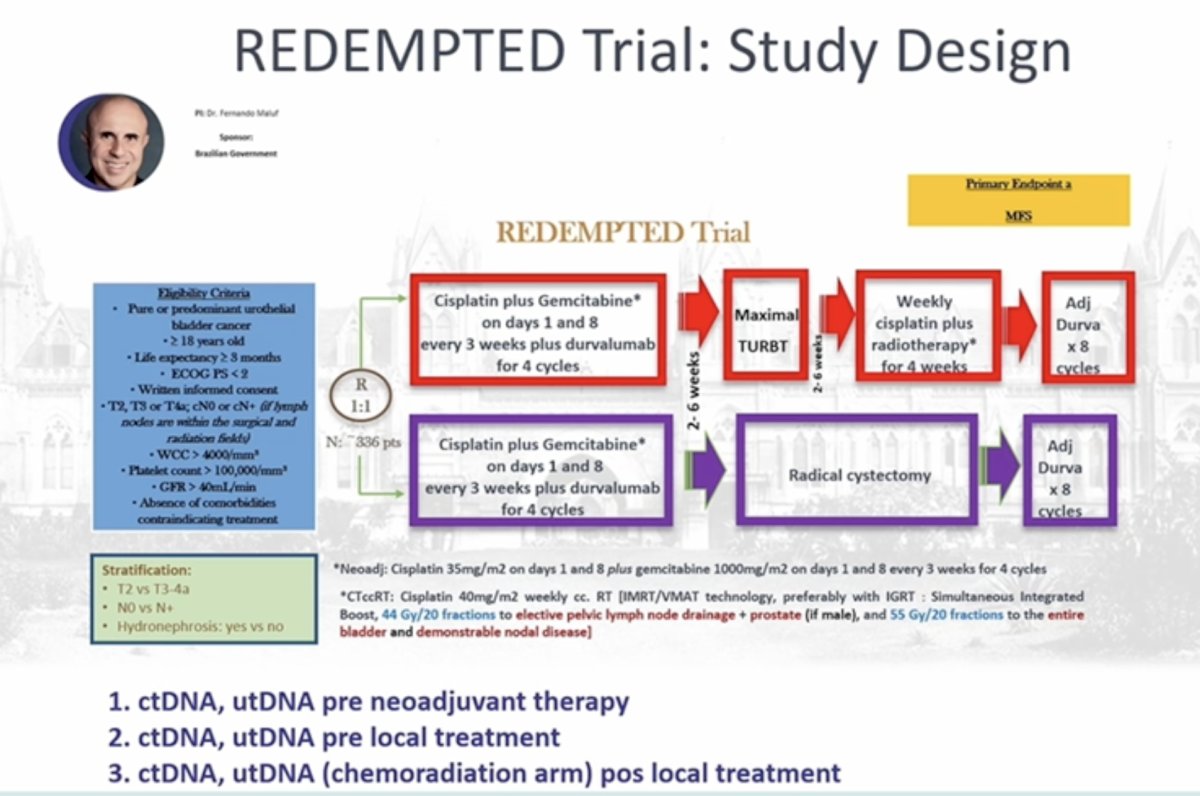
Dr. Maluf concluded by emphasizing that continued improvements in systemic therapy, imaging modalities, and molecular diagnostics are rapidly advancing the field toward more precise patient selection. Increasing rates of pCR with modern chemoimmunotherapy regimens, combined with advances in molecular minimal residual disease detection, may soon allow clinicians to accurately identify patients who have achieved true eradication of invasive disease. Integration of imaging, pathology, genomic profiling, ctDNA, and utDNA may ultimately enable clinicians to predict true pathologic complete response with a very high degree of confidence.
He summarized that these advances may allow clinicians to precisely select patients for bladder preservation strategies in the near future. As he concluded, progress in the field often begins by challenging long-standing assumptions, emphasizing that careful integration of emerging biomarkers and prospective trials may soon transform the management paradigm for patients with MIBC.
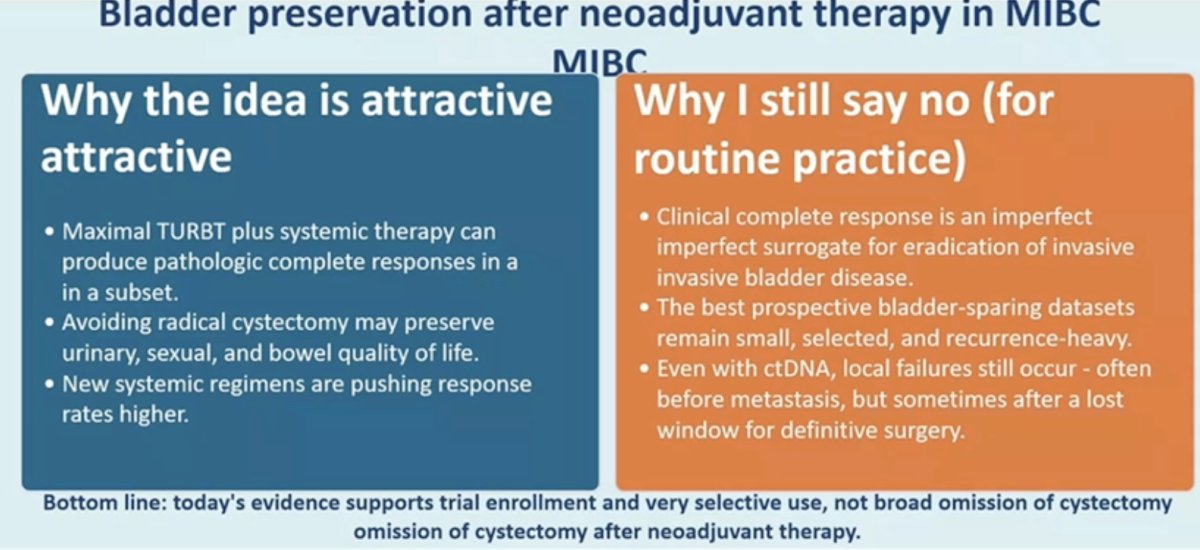
Next, Dr. Bogdana Schmidt argued that bladder preservation after NAC in muscle-invasive bladder cancer remains a risky proposition outside of carefully selected clinical trial settings.
She began by acknowledging why the concept is attractive. Maximal TURBT combined with systemic therapy can produce pCR in a subset of patients. Avoiding radical cystectomy may preserve urinary, sexual, and bowel function, and the emergence of more effective systemic regimens has increased interest in response-adapted strategies. However, Dr. Schmidt emphasized that cCR is an imperfect surrogate for the eradication of invasive disease. Prospective bladder-sparing datasets remain small and highly selected, and even when ctDNA is incorporated, local failures remain common. Importantly, these failures can occur before metastasis but sometimes after the optimal window for definitive cystectomy has passed. As a result, current evidence supports enrollment in clinical trials and highly selective use rather than routine omission of cystectomy following neoadjuvant therapy.
She then outlined several key unanswered questions that must be addressed before bladder preservation can be safely implemented in routine practice:
- WHO: Which patients are truly appropriate candidates for a bladder-preserving approach?
- WHAT: What defines a reliable complete responder following neoadjuvant therapy?
- HOW: What surveillance strategies are required to detect recurrence early?
- WHEN: How long must patients be monitored to ensure durable disease control?
- WHAT: What exactly constitutes “bladder preservation,” and what oncologic endpoints should define success?
To illustrate the long-term risks, Dr. Schmidt presented retrospective data from the Memorial Sloan Kettering Cancer Center evaluating 101 patients treated between 1994 and 2015 who achieved cCR after cisplatin-based neoadjuvant chemotherapy and maximal TURBT.7 These patients represented an “ideal” cohort: all had cT2 disease, solitary tumors ≤5 cm, and relatively favorable features, although 26% had concomitant CIS and 16% had lymphovascular invasion. Despite this favorable selection, long-term outcomes revealed substantial recurrence risk. At 15 years, 38% experienced bladder recurrence, including 9 cases of recurrent MIBC. Eleven percent ultimately required cystectomy, and bladder cancer–specific mortality reached 11%. Among those who developed bladder recurrence, the 5- and 15-year cancer-specific mortality rates were 15% (95% CI 4.7–26) and 26% (95% CI 14–41), respectively, highlighting that recurrence risk persists well beyond a decade.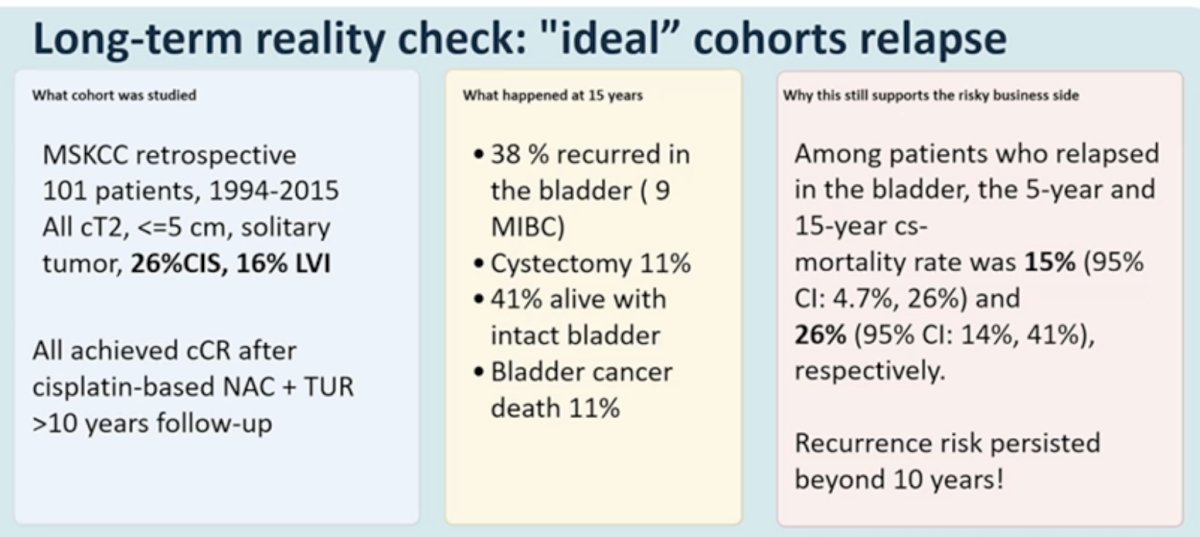
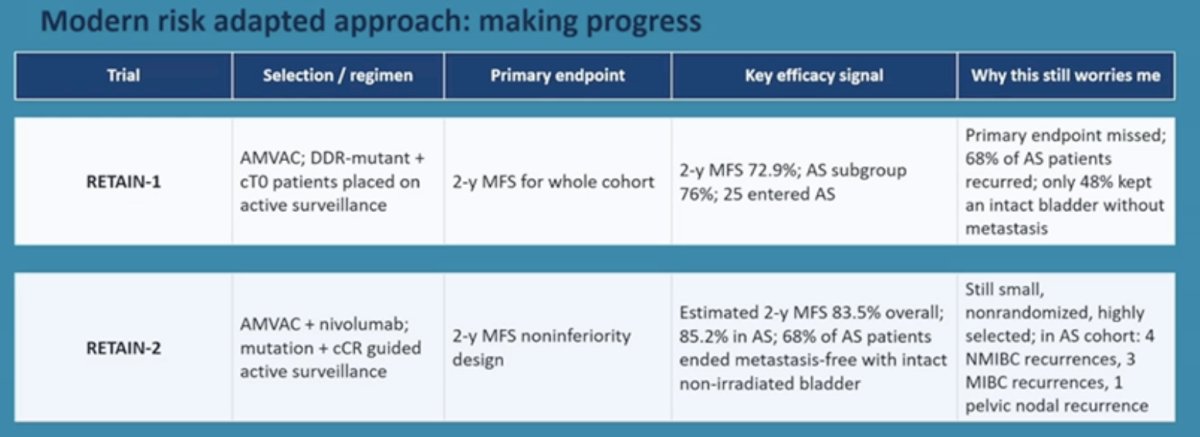
Dr. Schmidt next reviewed modern risk-adapted strategies designed to identify patients who might safely defer cystectomy. The RETAIN-1 study evaluated a biomarker-driven approach using accelerated MVAC chemotherapy, with DDR-mutant and clinical T0 patients entering active surveillance. The primary endpoint was 2-year metastasis-free survival for the entire cohort. Two-year MFS reached 72.9%, and in the active surveillance subgroup, it was 76%, with 25 patients entering surveillance. However, the study failed to meet its primary endpoint: 68% of patients on active surveillance experienced recurrence, and only 48% ultimately maintained an intact bladder without metastasis.
The RETAIN-2 trial incorporated nivolumab with accelerated MVAC and used ctDNA alongside clinical response to guide surveillance. In this study, the estimated 2-year MFS was 83.5% overall and 85.2% among those managed with active surveillance. However, the study remained small and nonrandomized, with highly selected patients. Even within the surveillance cohort, recurrences still occurred, including non–muscle-invasive recurrences (n=4), muscle-invasive recurrences (n=3), and one pelvic nodal recurrence.
Among 22 patients managed with active surveillance in these trials, outcomes demonstrated the complexity of this strategy. Fourteen patients remained recurrence-free, but recurrences included four NMIBC recurrences, three MIBC recurrences, and one pelvic nodal recurrence. Several patients required salvage cystectomy or chemoradiation, underscoring the dependence of this approach on timely detection and successful salvage therapy.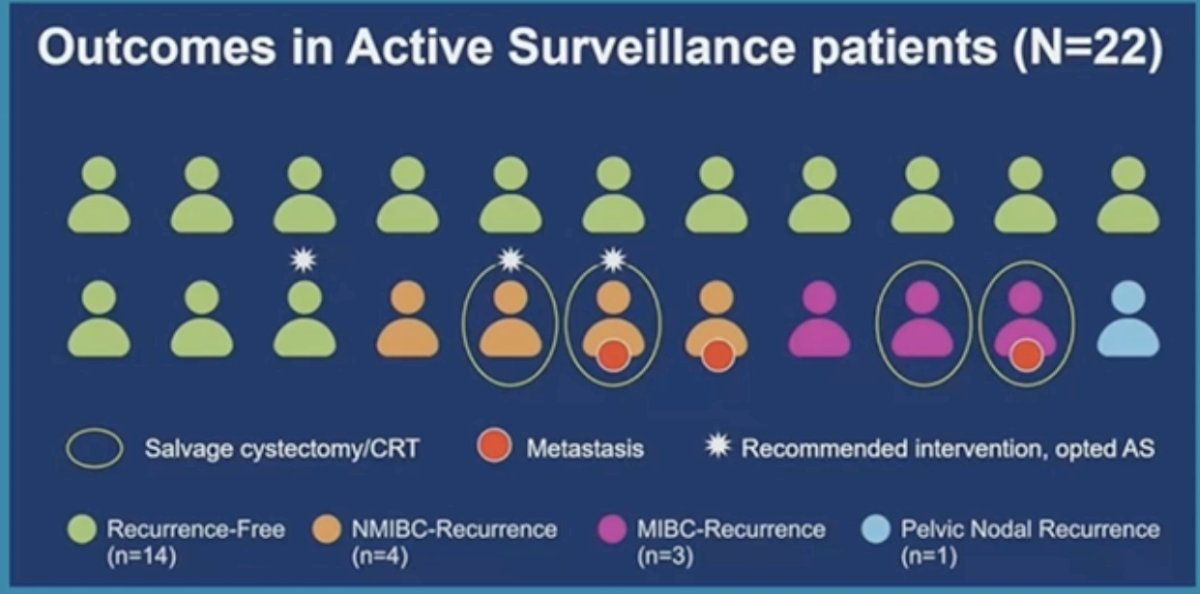
A comparison of outcomes between RETAIN-1 and RETAIN-2 further illustrates the ongoing uncertainty. In RETAIN-1, local recurrence occurred in 62% of patients and metastases developed in 36%, while only 48% remained metastasis-free with an intact non-irradiated bladder. In RETAIN-2, local recurrence rates were lower at 36%, metastases occurred in 14%, and 68% of patients remained metastasis-free with an intact bladder. Dr. Schmidt noted that these improvements may reflect better systemic therapy or improved selection, but they still fall short of demonstrating that cystectomy can be safely omitted.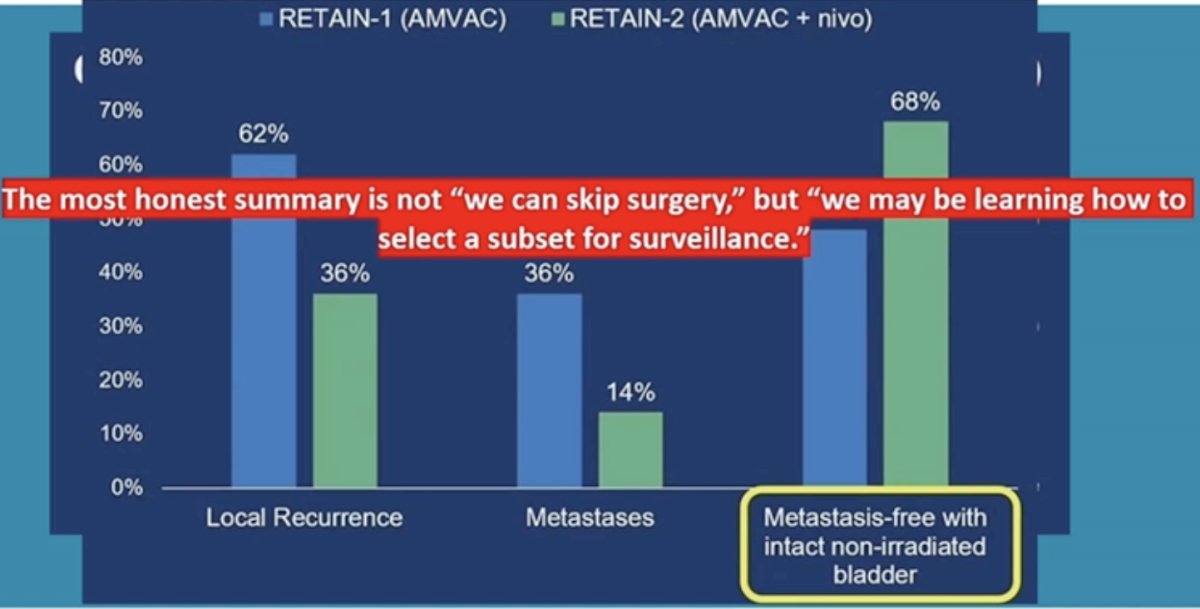
She then discussed the SURE-02 trial, a single-center phase II study evaluating sacituzumab govitecan combined with pembrolizumab in cisplatin-ineligible or cisplatin-refusing patients.8 Among 49 treated patients with a median follow-up of 14 months, the clinical complete response rate was 39% (19/49). While all cCR patients were metastasis-free at data cutoff, two developed intravesical relapse, and six patients developed distant metastases. Dr. Schmidt cautioned that these results are promising but fragile: the study was single-arm, conducted at a single center, and follow-up remains short. Moreover, even among patients achieving cCR, bladder relapses still occurred.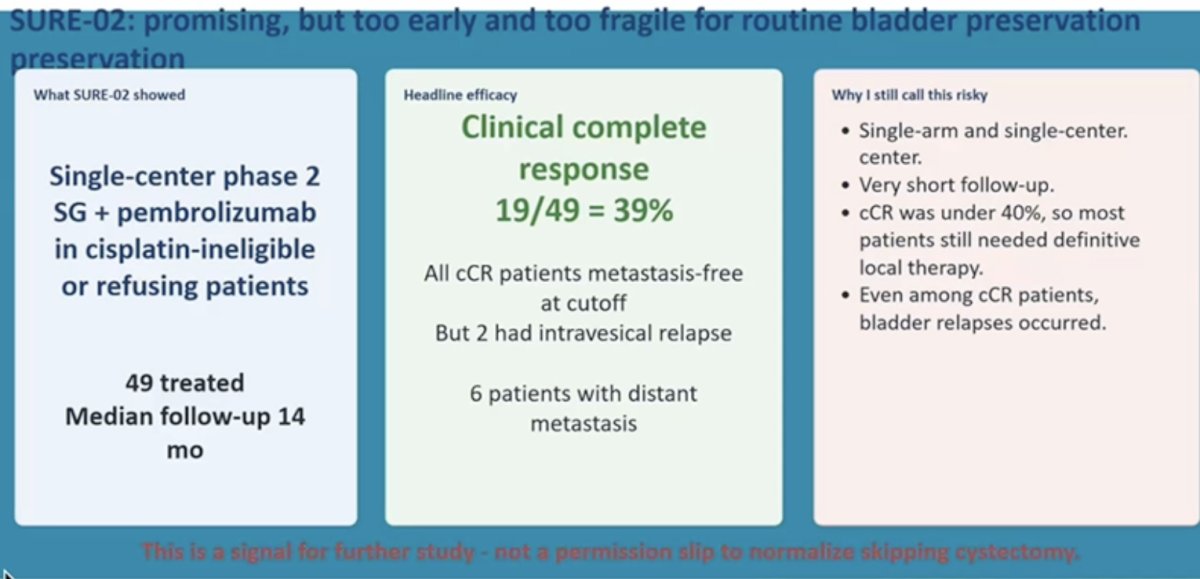
She also addressed the emerging role of EV+P. In the phase III EV-304 trial in cisplatin-eligible patients, EV+P improved EFS and overall survival compared with gemcitabine/cisplatin and increased the pCR rate to 55.8% versus 32.5%. However, these pCR data were generated in the context of timely radical cystectomy. As such, a pCR at surgery does not necessarily validate a bladder-preservation strategy based on clinical response alone.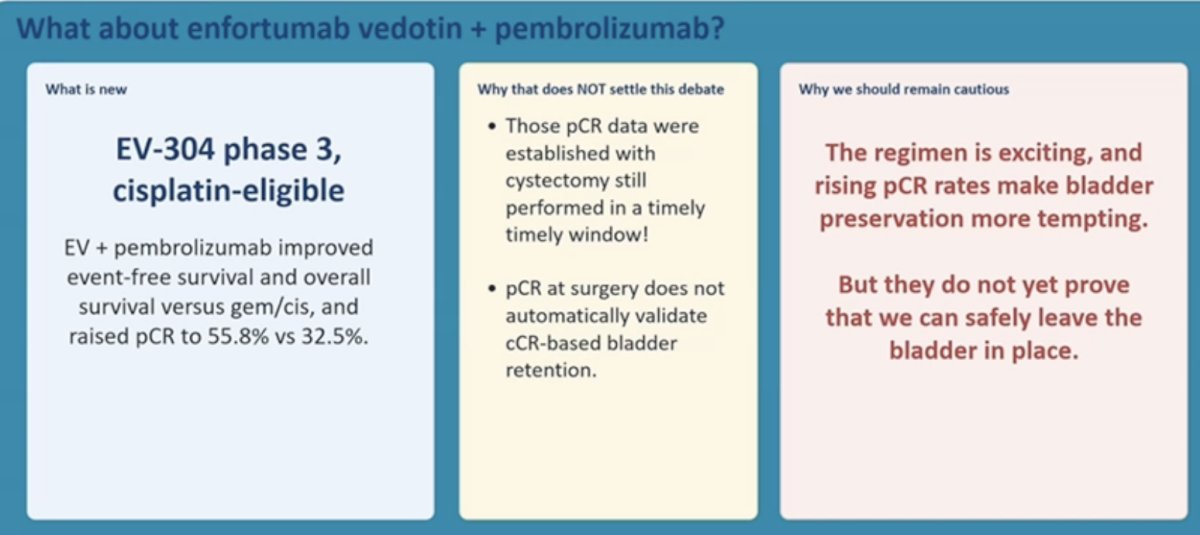
Dr. Schmidt emphasized that the central problem remains the disconnect between clinical complete response and durable local control. For bladder preservation to be safely implemented, several conditions must be met. Restaging must reliably exclude residual invasive disease within the bladder. Biomarkers must accurately identify patients cured both locally and systemically. Salvage pathways must preserve outcomes if local recurrence occurs. At present, these criteria are not fully satisfied.
Data from the RETAIN program highlight the limitations of ctDNA. While ctDNA appears useful for detecting metastatic risk, it does not reliably predict local bladder recurrence. Among 21 local recurrences in RETAIN-2 active surveillance patients, only two were ctDNA+. Moreover, all metastatic events in the active surveillance cohort were preceded by local recurrence, underscoring the importance of vigilant bladder-directed surveillance.
These findings carry important practical implications. A negative ctDNA test cannot replace direct bladder assessment. Surveillance strategies must be intensive and multimodal, incorporating cystoscopy, imaging, and molecular tools. Missing early invasive regrowth could eliminate the best opportunity for curative surgery.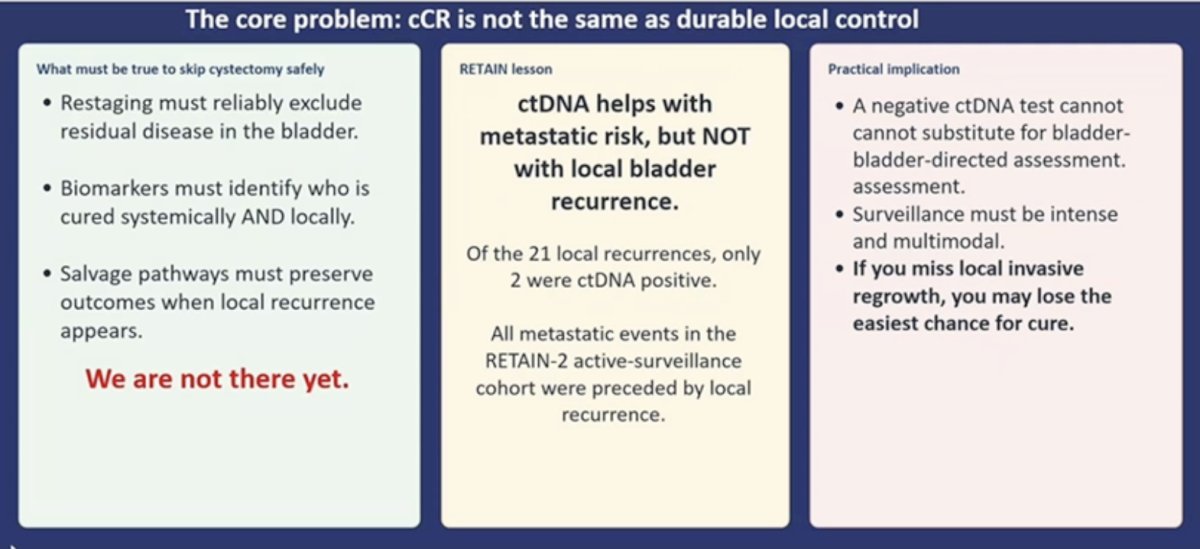
Dr. Schmidt concluded that bladder preservation after neoadjuvant therapy without bladder-directed radiotherapy remains investigational. Trials such as RETAIN and SURE-02 demonstrate that some patients may avoid immediate cystectomy, but this strategy comes with persistent uncertainty regarding residual disease, substantial recurrence risk, and heavy reliance on intensive surveillance and successful salvage therapy.
Until several key requirements are met—including clear criteria for patient selection, standardized definitions of complete response, mature prospective data demonstrating durable bladder-intact survival, validated surveillance strategies, and well-defined salvage outcomes—routine omission of cystectomy following neoadjuvant therapy should be approached cautiously. She reiterated that, outside of clinical trials, bladder preservation in this context remains risky business.
Presented By:
- Benjamin Pradere, MD, MSc, Professor, Attending Urologist, Clinique La Croix du Sud, Quint Fonsegrives, France
- Fernando Maluf, MD, PhD, Chief of Medical Oncology at the Beneficencia Portuguesa, Steering Committee Member, Medical Oncology Center at Albert Einstein Hospital, São Paulo, Brazil
- Bogdana Schmidt, MD, MPH, Assistant Professor of Urology, Department of Urology, University of Utah, Salt Lake City, UH
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the EAU 2026 Annual Congress, London, UK, March 13th–16th, 2026
References:- Powles T, Catto JWF, Galsky MD, et al. Perioperative durvalumab with neoadjuvant chemotherapy in operable bladder cancer. N Engl J Med. 2024;391(19):1773–1786.
- Vulsteke C, Adra N, Danchaivijitr P, et al. Perioperative Enfortumab Vedotin and Pembrolizumab in Bladder Cancer. N Engl J Med. 2026.
- Neoadjuvant and adjuvant enfortumab vedotin plus pembrolizumab for participants with muscle-invasive bladder cancer who are eligible for cisplatin: randomized open-label phase 3 KEYNOTE-B15 study. UroToday. 2026. Available at: https://www.urotoday.com/conference-highlights/asco-gu-2026/asco-gu-2026-bladder-cancer/166943-asco-gu-2026-neoadjuvant-and-adjuvant-enfortumab-vedotin-pembrolizumab-for-participants-with-mibc-who-are-eligible-for-cisplatin-randomized-open-label-phase-3-keynote-b15-study.html
- Galsky MD, Daneshmand S, Izadmehr S, et al. Gemcitabine and cisplatin plus nivolumab as organ-sparing treatment for muscle-invasive bladder cancer: a phase 2 trial. Nat Med. 2023;29(11):2825–2834. doi:10.1038/s41591-023-02568-1.
- Young MN, Szabados B, Assaf Z, et al. Predictive value of dynamic changes in ctDNA and baseline biomarkers with neoadjuvant atezolizumab in operable urothelial carcinoma in the ABACUS trial. J Clin Oncol. 2024;42(4_Suppl).
- Ghatalia P, Ross E, Zibelman MR, et al. A phase 2 trial of risk enabled therapy after neoadjuvant chemo-immunotherapy for muscle-invasive bladder cancer (RETAIN-2). J Clin Oncol. 2026;43(5_Suppl).
- Donat SM, Tin AL, Vickers AJ, Herr H. Neoadjuvant Chemotherapy With Transurethral Resection for Bladder Preservation: 15-Year Follow-Up of the Retained Bladder. J Urol. 2025;214(6):591-600.
- Necchi A, de Jong JJ, Proudfoot JA, et al. Neoadjuvant sacituzumab govitecan (SG) plus pembrolizumab (Pembro), followed by response-adapted bladder sparing and adjuvant pembro, in patients with muscle-invasive bladder cancer (MIBC): SURE-02 primary analysis and biomarker results. J Clin Oncol. 2026;44(7_Suppl).