(UroToday.com) The 2026 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Matthew Galsky discussing results from the randomized, open-label, phase 3 KEYNOTE-B15 study assessing neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab for participants with muscle invasive bladder cancer who are eligible for cisplatin. Radical cystectomy is a standard treatment for muscle invasive bladder cancer. However, despite radical cystectomy, approximately 50% of patients still develop metastatic recurrence. As such, systemic therapy administered prior to cystectomy (ie, neoadjuvant therapy) could theoretically eradicate microscopic disease and prevent recurrence. There has been a paucity of advances in neoadjuvant therapy for muscle invasive bladder cancer, dating back to cisplatin-based neoadjuvant therapy improving survival1,2 in the early 2000’s. Moreover, based on the EV-302 trial,3 enfortumab vedotin + pembrolizumab is now standard of care for patients with metastatic bladder cancer. In the KEYNOTE-B15 trial, Dr. Galsky and colleagues compared enfortumab vedotin + pembrolizumab and cystectomy versus cisplatin + gemcitabine and cystectomy for the treatment of muscle invasive bladder cancer.
In KEYNOTE-B15, adult patients with muscle invasive bladder cancer (clinical T2-T4aN0M0 or T1-T4aN1M0), predominantly urothelial histology (>50%), and candidates for a radical cystectomy + pelvic lymph node dissection were eligible for the trial. Additionally, patients had to not meet any Galsky criteria for cisplatin ineligibility and have an ECOG performance status of 0-1. Patients were then randomized 1:1 to enfortumab vedotin 1.25 mg/kg day 1 and day 8 IV Q3W for 4 cycles + pembrolizumab 200 mg day 1 IV Q3W for 4 cycles versus cisplatin 70 mg/m2 day 1 IV Q3W for 4 cycles + gemcitabine 1000 mg/m2 day 1 and day 8 IV Q3W for 4 cycles followed by radical cystectomy + pelvic lymph node dissection for all patients. Following surgery, patients in the enfortumab vedotin + pembrolizumab arm continued on 5 maintenance cycles of enfortumab vedotin + 13 cycles of maintenance pembrolizumab, whereas patients in the cisplatin + gemcitabine arm underwent observation. The trial design for KEYNOTE-B15 is as follows:
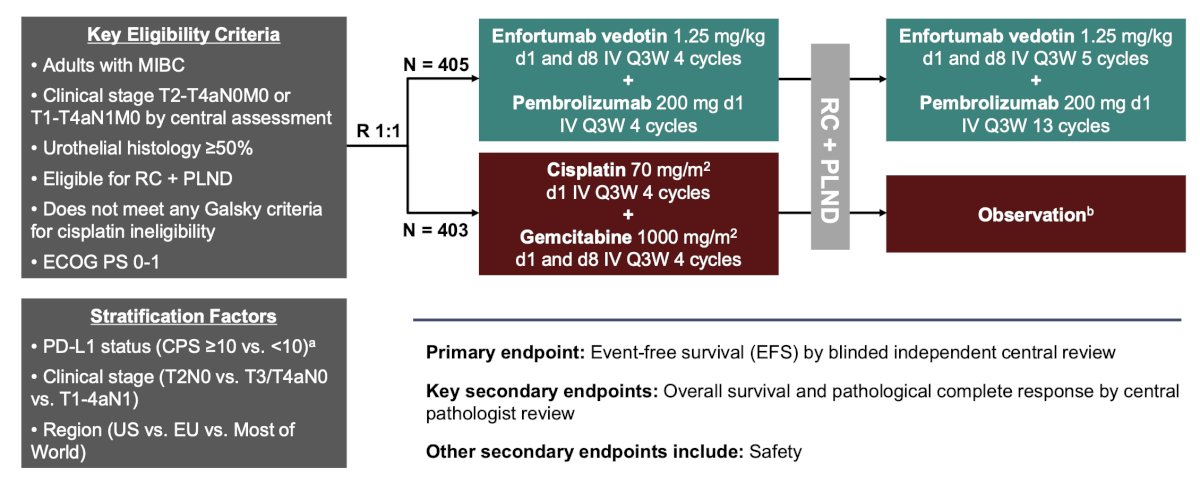
The primary endpoint was event free survival by blinded independent central review, and key secondary endpoints included overall survival and pathological complete response by central pathologist review. Other secondary endpoints included safety.
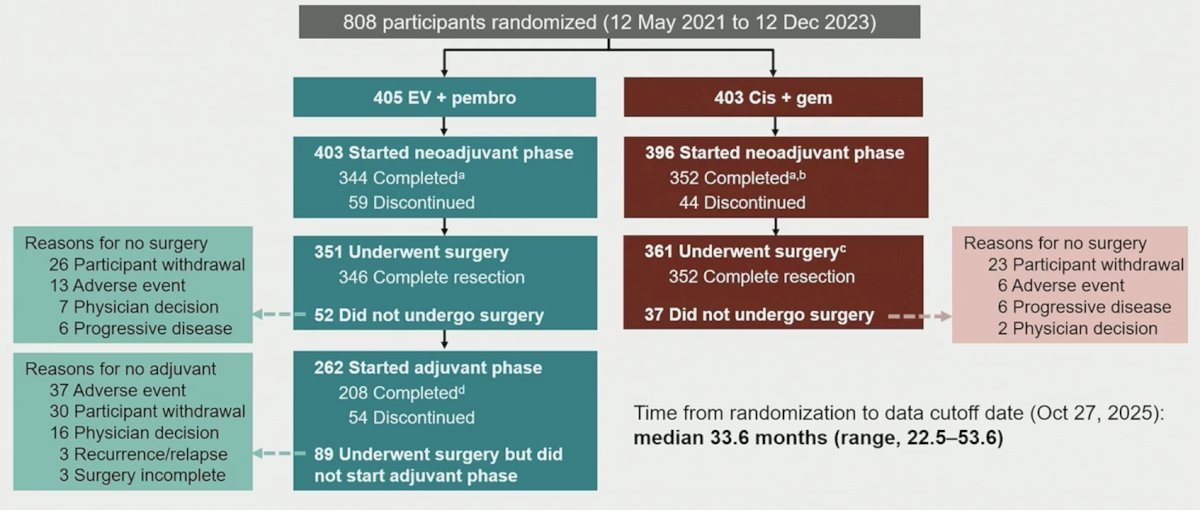
There were 808 patients randomized from May 12, 2021, to December 12, 2024, including 405 to enfortumab vedotin + pembrolizumab and 403 to cisplatin + gemcitabine. The patient disposition is as follows:
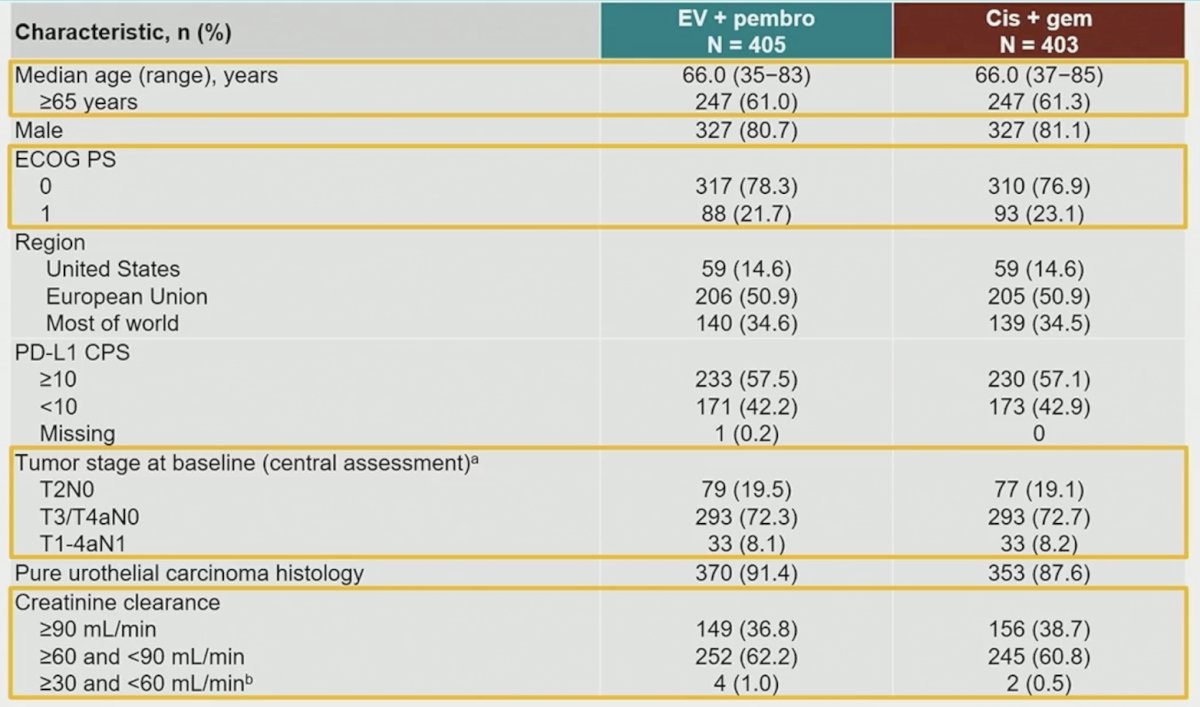
Baseline demographics for the patients in the trial were well balanced between the two arms:
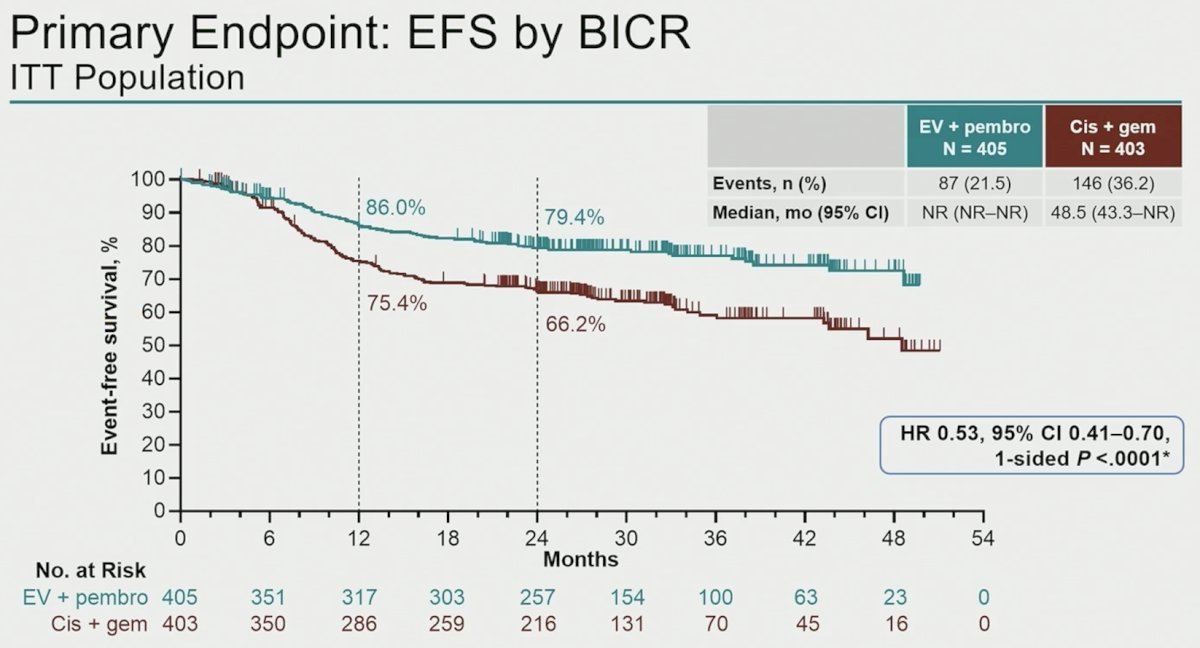
The study met its primary endpoint of improving event free survival, with a median not reached (95% CI not reached to not reached) for enfortumab vedotin + pembrolizumab and 48.5 months (95% 43.3 to not reached) for cisplatin + gemcitabine (HR 0.53, 95% CI 0.41-0.70; p < 0.0001). The 12 month event free survival rate for enfortumab vedotin + pembrolizumab was 86.0% versus 75.4% for cisplatin + gemcitabine, and the 24 month rate was 79.4% for enfortumab vedotin + pembrolizumab versus 66.2% for cisplatin + gemcitabine:
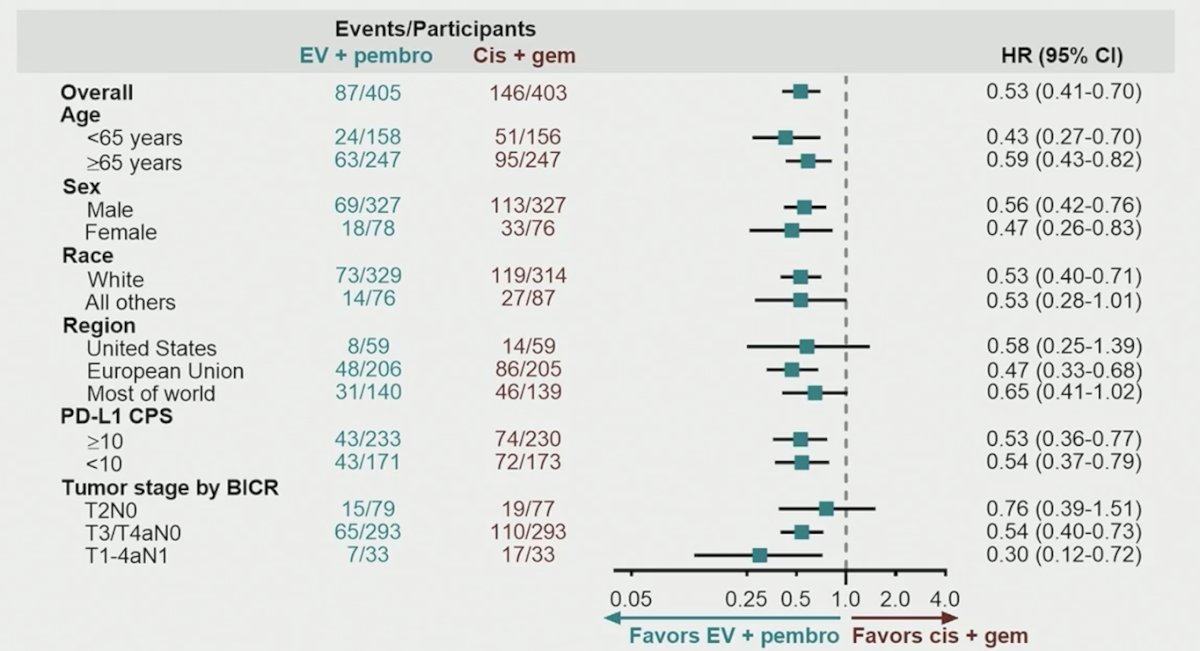
Regarding the event free survival subgroups, there was a consistent benefit favoring enfortumab vedotin + pembrolizumab:
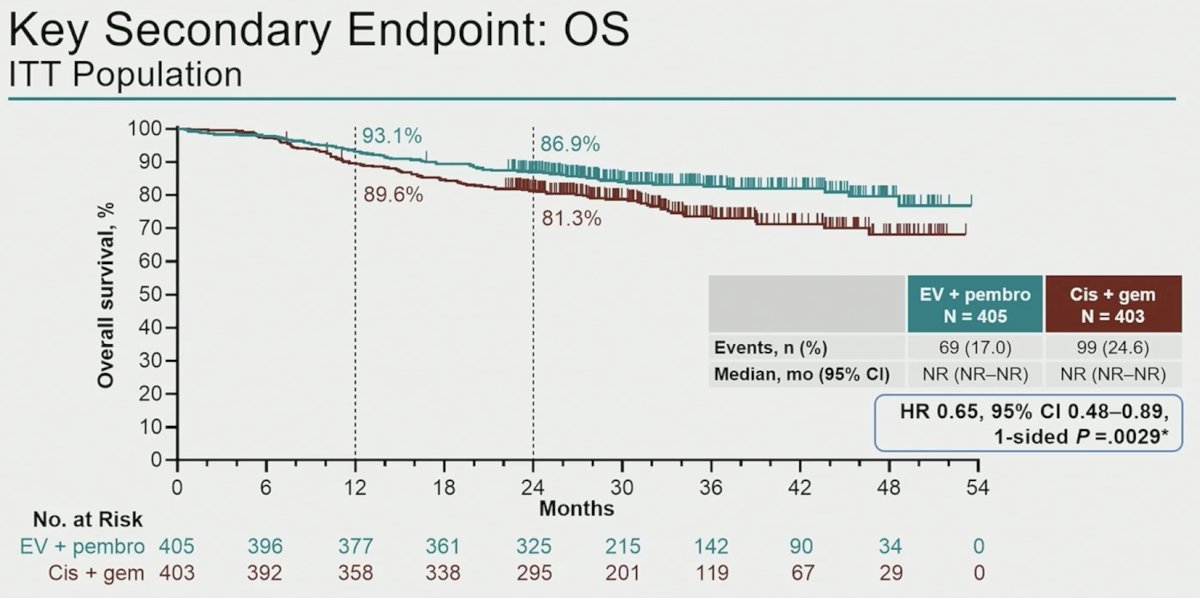
The median overall survival was not reach in either arm, with the hazard ratio favoring enfortumab vedotin + pembrolizumab: HR 0.65, 95% CI 0.48-0.89; p = 0.0029. The 12 month overall survival rate was 93.1% for enfortumab vedotin + pembrolizumab versus 89.6% for cisplatin + gemcitabine, with a 24 month rate of 86.9% and 81.3%, respectively:
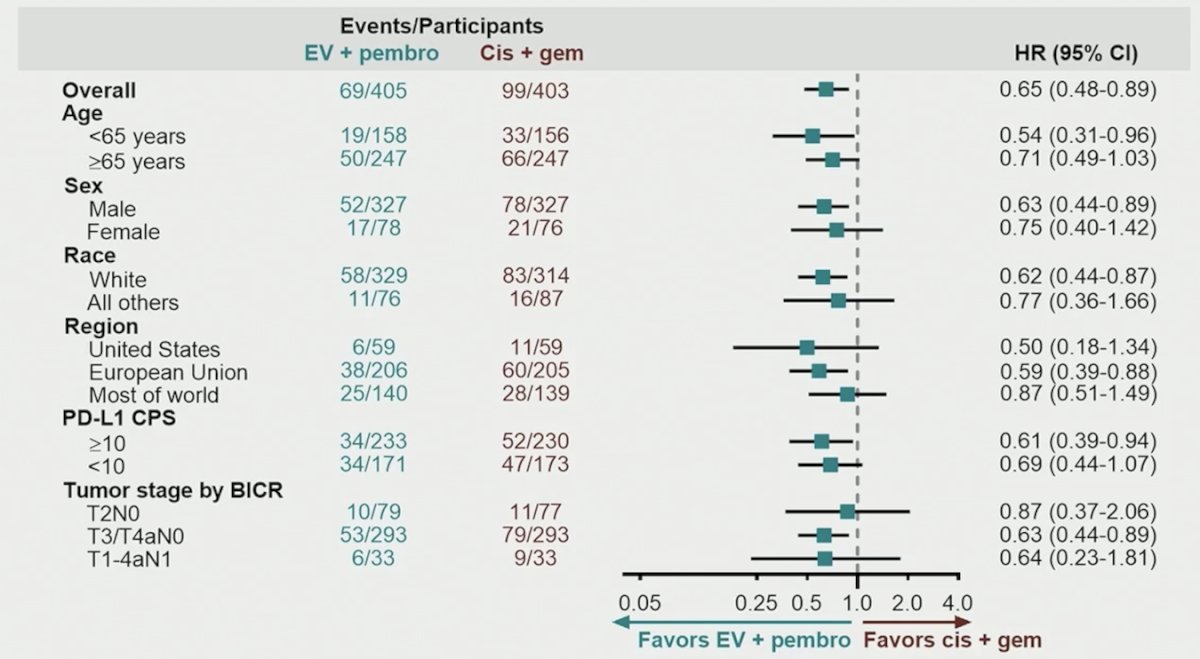
Similar to event free survival, the overall survival subgroup analysis favored the enfortumab vedotin + pembrolizumab patients:
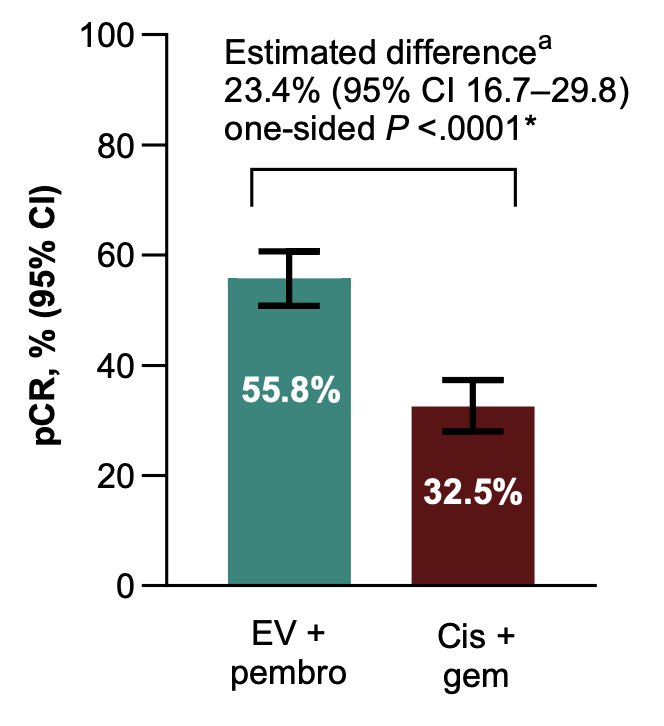
The pathological complete response rate for enfortumab vedotin + pembrolizumab was 55.8% versus 32.5% for cisplatin + gemcitabine, with an estimated difference of 23.4% (95% CI 16.7 – 29.8; p < 0.001):
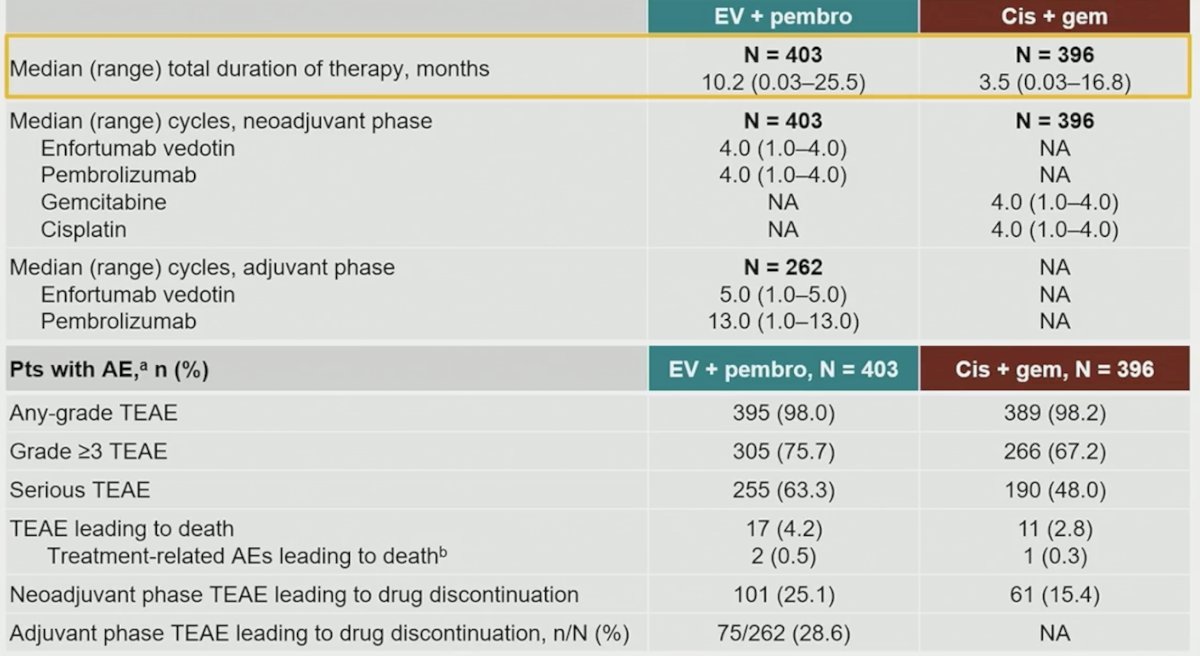
The median total duration of therapy was 10.2 months (range: 0.03-25.5) for patients receiving enfortumab vedotin + pembrolizumab compared to 3.5 months (range: 0.03-16.8) for patients receiving cisplatin + gemcitabine. With regards to safety, grade 3+ treatment emergent adverse events occurred in 75.7% of patients in the enfortumab vedotin + pembrolizumab arm versus 67.2% in the cisplatin + gemcitabine arm:
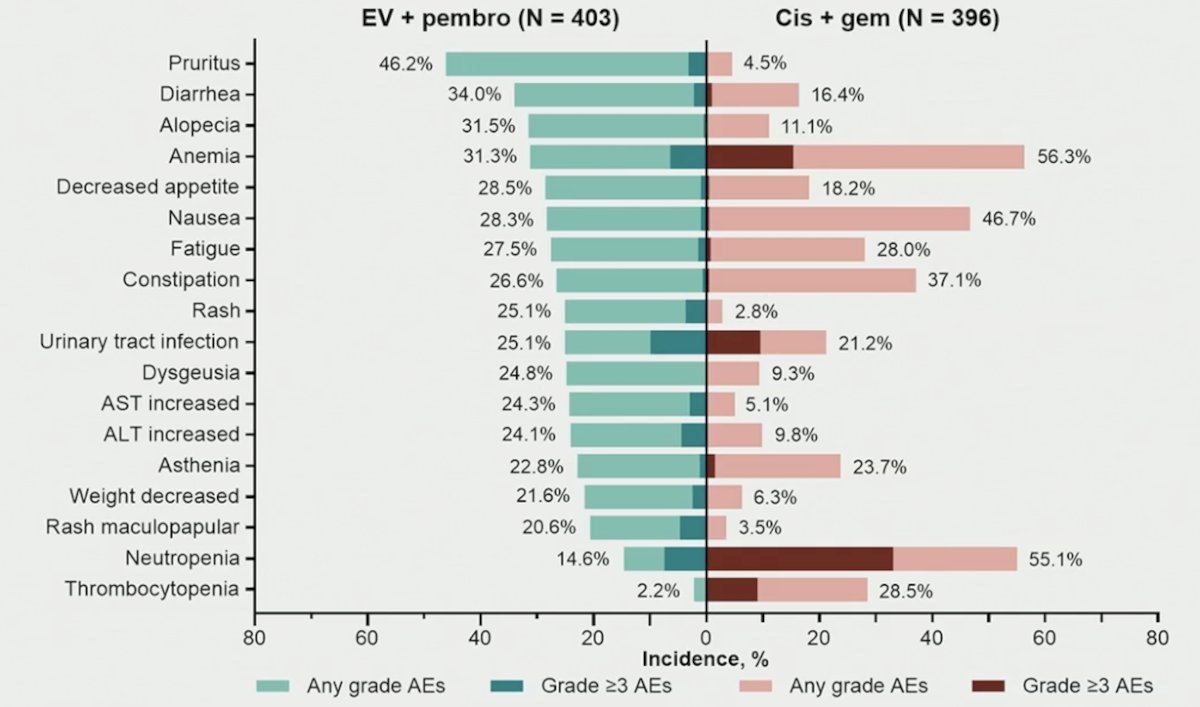
The most common treatment emergent adverse event (incidence >=20% in either arm) was pruritus (46.2%) in the enfortumab vedotin + pembrolizumab arm and anemia (56.3%) in the cisplatin + gemcitabine arm:
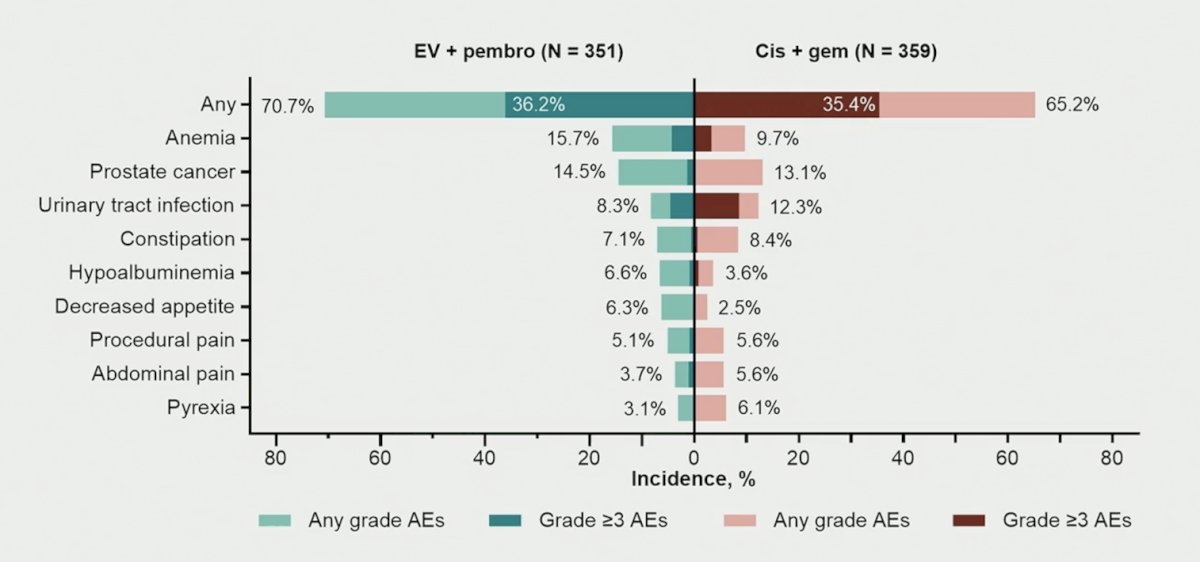
With regards to treatment emergent adverse events during the surgery phase, 70.7% of patients in the enfortumab vedotin + pembrolizumab arm had an event versus 65.2% in the cisplatin + gemcitabine arm. The most common treatment emergent adverse event in the enfortumab vedotin + pembrolizumab arm was anemia (15.7%), and prostate cancer (13.1%) in the cisplatin + gemcitabine arm:
Dr. Galsky concluded his presentation discussing results from the randomized, open-label, phase 3 KEYNOTE-B15 study with the following take-home points:
- Neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab significantly improved event free survival, overall survival, and pathological complete response rate versus neoadjuvant gemcitabine + cisplatin in patients with muscle invasive bladder cancer who are eligible for cisplatin-containing therapy and radical cystectomy
- The safety profile of neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab was consistent with prior experience with this combination regimen
- Enfortumab vedotin + pembrolizumab represents the first antibody drug conjugate + immune checkpoint inhibitor combination to improve outcomes versus cisplatin-based chemotherapy in patients with muscle invasive bladder cancer eligible for curative intent surgery and cisplatin-containing therapy
- The KEYNOTE-905 study recently showed this regimen improved outcomes versus cystectomy alone in “cisplatin-ineligible” patients
- The KEYNOTE-B15 study, coupled with the recently reported results from the KEYNOTE-905 study, supports neoadjuvant and adjuvant enfortumab vedotin + pembrolizumab (+ cystectomy) as a treatment option for patients with muscle invasive bladder cancer, regardless of cisplatin-eligibility
Presented by: Matthew D. Galsky, MD, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References:
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med 2003;349(9):859-866.
- Griffiths G, Hall R, Sylvester R, et al. International phase III trial assessing neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive bladder cancer: long term results of the BA06 30894 trial. J Clin Oncol 2011;29(16):2171-2177.
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024 Mar 7;390(10)875-888.