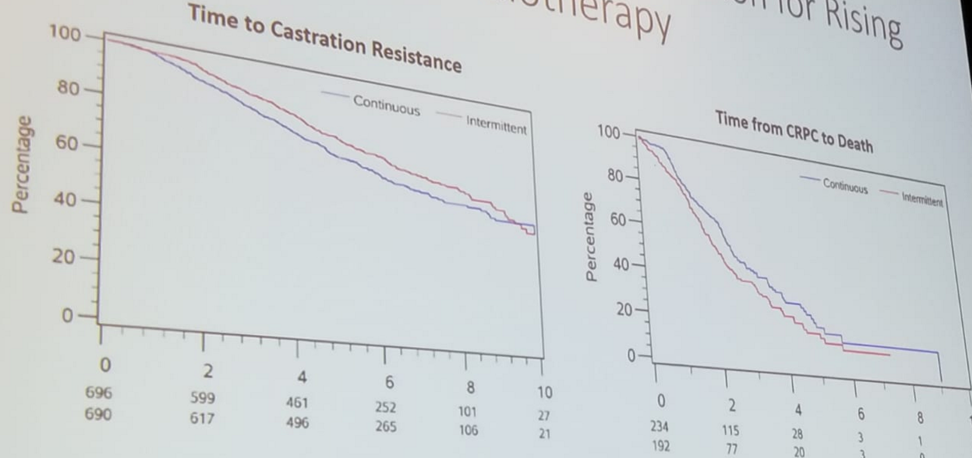
Figure 1 - Intermittent ADT was not inferior to continuous ADT for rising PSA after radiotherapy of prostate cancer
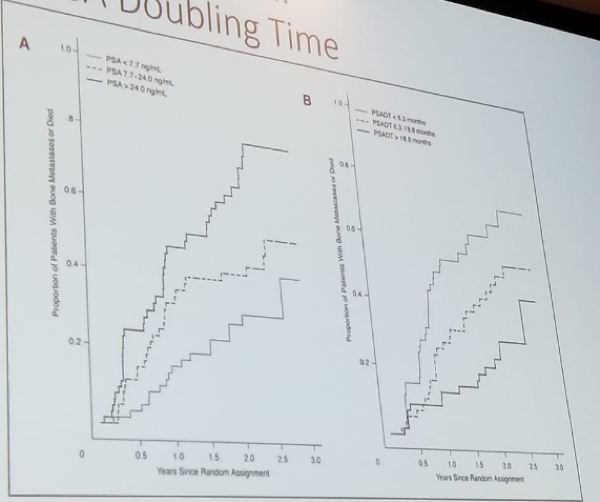
The value of total PSA and PSA doubling time (DT) also has a tremendous effect on the proportion of patients developing bone metastasis or dying from the disease (figure 2).2
Figure 2 – Effect of PSA and PSA doubling time on bone metastasis:
For patients transitioning to the status of CRPC, some “vintage” 2nd line hormonal therapies include:
- Addition/changing of non-steroidal anti-androgen (NSAA)
- Withdrawal of NSAA
- Addition of corticosteroids
- Addition of Ketoconazole
- Addition of Estrogen
Figure 3 – The STRIVE study: Progression-free survival - Enzalutamide vs. Bicalutamide:

Most recently, the PROSPER study [5], showed a clear advantage when M0 CRPC patients were treated with enzalutamide, compared to placebo, in terms of:
- Metastasis-free survival (MFS) (figure 4)
- Time to PSA progression
- Time to use of new antineoplastic therapy
- PSA response

Another recently reported study is the SPARTAN trial comparing Apalutamide to Placebo in M0 CRPC patients.6 Like the PROSPER trial, this trial showed a similar advantage to treatment with Apalutamide, when compared to placebo, in terms of MFS (Figure 5).
Figure 5 – MFS in Apalutamide vs. Placebo:

Chi concluded his overview by mentioning some important controversies and considerations. The 1st point is that it is difficult to extrapolate all these data to all M0 patients. Most patients analyzed were very high risk, with a PSA doubling time of fewer than 6 months (high risk is defined as PSA doubling time of fewer than 10 months). Another important point is that MFS is apparently a clinically meaningful and worthwhile endpoint. Furthermore, in these trials, there was no difference in the OS between the different treatment arms. This could be due to cross-over and subsequent treatment in the placebo arms, or because disease progression is different, because of androgen-resistant CRPC. Additionally, the quality of life won’t be able to get better, and if anything, it is just going to get worse, due to treatment toxicity.
Some additional important points included the addition of PSMA PET scans into the standard of care. This could totally re-stratify no-metastatic patients as metastatic patients, and change their allocation, and might even improve the outcomes. Lastly, we need to consider the evolving management of oligometastasis.
In summary, patients with M0 CRPC and short PSA doubling time (<6 months) are at higher risk of developing metastasis. In Canada, there is currently no approved treatment for M0 CRPC patients, and Denosumab and zoledronic acid are not indicated. The most recent trials (PROSPER, and SPARTAN) have demonstrated that both Apalutamide and Enzalutamide demonstrate substantial benefits in MFS and other progression events. To date, these trials do not show any OS benefit, and the decision to treat should be individualized and restricted to high-risk patients only.
References:
1. J Crook et al. N Engl J Med 2012; 367:895-903
2. MR Smith, et al. J Clin Oncol, 23:2918, 2005
3. MR Smith, et al. Lancet; 379(9810): 39-46, 2012
4. DF Penson, et al. J Clin Oncol, 34; 2098-2106, 2016
5. M Hussain, et al. J Clin Oncol 36, 2018 (suppl 6s; abstr 3)
6. MR Smith, et al. N Engl J Med 2018; 378:1408-1418
Presented by: Kim Chi, MD, University of British Columbia, Vancouver, Canada
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, @GoldbergHanan at the 73rd Canadian Urological Association Annual Meeting - June 23 - 26, 2018 - Halifax, Nova Scotia