(UroToday.com) The 2026 AUA annual meeting featured the International Prostate Forum and a presentation by Dr. Tarik Esen discussing the role of lymph node dissection at the time of radical prostatectomy. In 2023, the EAU guidelines stated that for intermediate risk prostate cancer, urologists should perform an extended pelvic lymph node dissection based on predicted lymph node invasion (validated nomogram).
However, in the 2026 EAU guidelines, there are more tempered recommendations, including offering radical prostatectomy to patients with a life expectancy of >10 years, and not mandating pelvic lymph node dissection, but if done, it should be performed as an extended pelvic lymph node dissection.
In 2017, Fossati and colleagues1 performed a systematic review to assess the benefits and harms of different extents of lymph node dissection during radical prostatectomy. Among 66 studies and including 275,269 patients, there was no significant difference in survival observed between the extent of lymph node dissection. Thus, at the time, the conclusion was that a direct therapeutic benefit is still not evident in the literature.
In 2021, Lestingi et al.2 published the early oncological outcomes of the only randomized phase 3 trial to date assessing extended versus limited pelvic lymph node dissection.2 In this trial, 300 patients were randomized at a single Brazilian center to extended versus limited pelvic lymph node dissection. The median biochemical recurrence-free survival was 61.4 months in the limited pelvic lymph node dissection group and not reached in the extended pelvic lymph node dissection group (HR 0.91, 95% CI 0.63-1.32; p = 0.6). Median metastasis-free survival was not reached in either group (HR 0.57, 95% CI 0.17-1.8; p = 0.3). In exploratory subgroup analysis, patients with preoperative biopsy ISUP grade groups 3-5 who were allocated to extended pelvic lymph node dissection had better biochemical recurrence-free survival (HR 0.33, 95% CI 0.14-0.74, interaction p = 0.007).
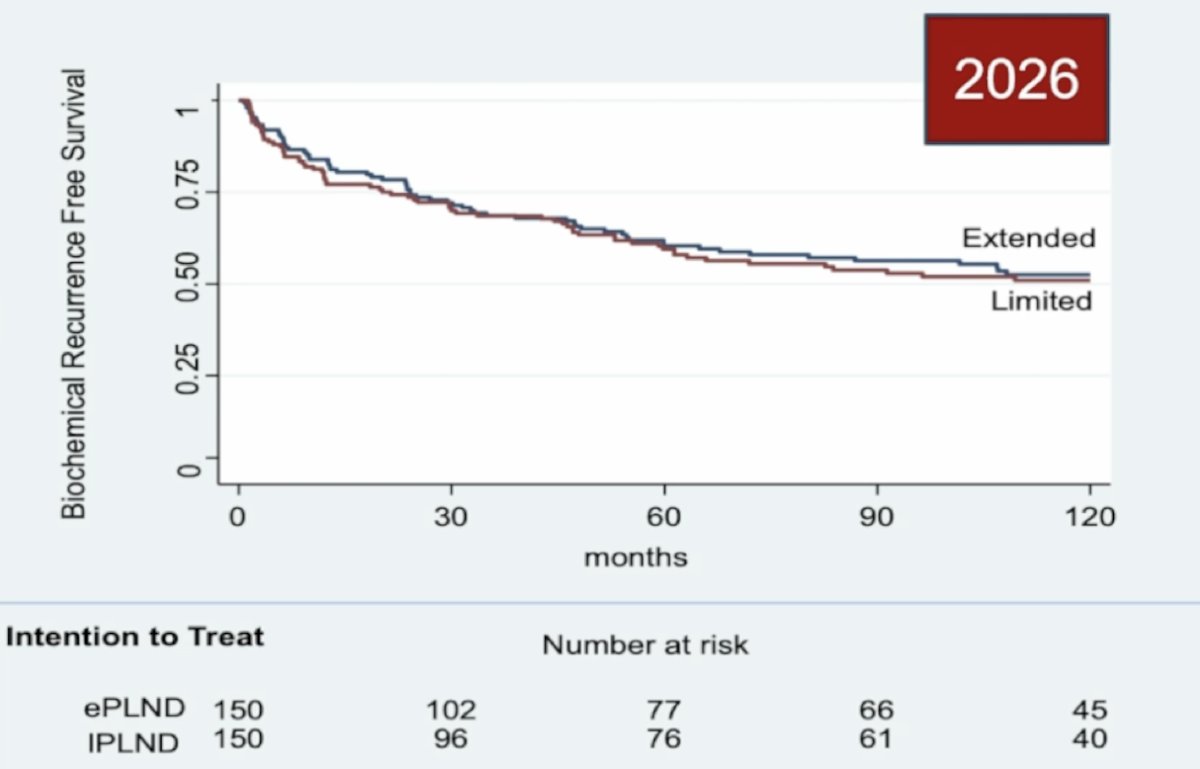
An update to this trial was presented by Dr. Lestingi at AUA 2026. With a mean and median follow-up of 119 (+/- 37.2) months and 130.6 (IQR 107.8-146.5) months, respectively, in the whole cohort, there was no difference in biochemical recurrence rates between the arms (HR 0.92, 95% CI 0.66-1.29; p = 0.638):
Additionally, patients with preoperative biopsy ISUP grade groups 3–5 who underwent extended pelvic lymph node dissection had better biochemical recurrence-free survival (HR 0.54, 95% CI 0.29-0.99; p =0.046):

In this high-grade subgroup, a significant improvement in metastasis-free survival was also observed with extended pelvic lymph node dissection (HR 0.26, 95% CI 0.07–0.93; p = 0.026) with extended follow-up:

In 2021, Touijer et al.3 published results of the Memorial Sloan Kettering Cancer Center randomized trial of limited versus extended pelvic lymph node dissection. Between October 2011 and March 2017, 1,440 men were randomized to limited (external iliac nodes) or extended (external iliac, obturator fossa, and hypogastric nodes) pelvic lymph node dissection, with a primary endpoint of biochemical recurrence. The median number of nodes retrieved was 12 (IQR 8-17) for limited pelvic lymph node dissection and 14 (IQR 10-20) for extended pelvic lymph node dissection. The corresponding rate of positive nodes was 12% and 14% (difference -1.9%, 95% CI -5.4% to 1.5%; p = 0.3). With a median follow-up of 3.1 years, there was no significant difference in the rate of biochemical recurrence between the groups (HR 1.04, 95% CI 0.93-1.15; p = 0.5):
Rates for grade 2 and 3 complications were similar at 7.3% for limited versus 6.4% for extended pelvic lymph node dissection, and there were no grade 4 or 5 complications.
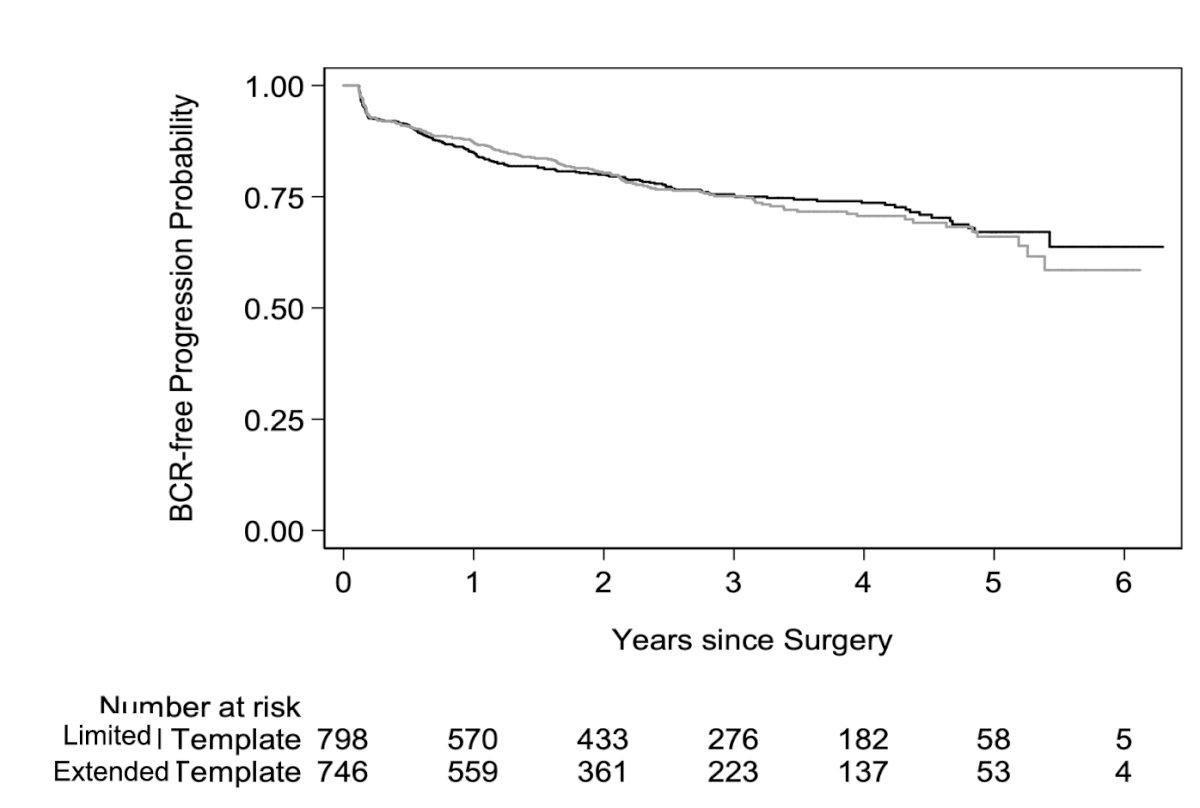
Updated follow-up for this Brazilian trial in 20254 reported that there were 452 biochemical recurrence events at a median follow-up of 4.2 years. The results confirmed the previous finding of comparable biochemical recurrence rates between the arms (HR 1.05, 95% CI 0.97-1.13; p = 0.30). However, with 123 metastasis events and a median follow-up of 5.4 years for patients without metastasis, they found a clinically and statistically significant protective effect of extended pelvic lymph node dissection against metastasis (any metastasis: HR 0.82, 95% CI 0.71-0.93; p = 0.003; distant metastasis: HR 0.75, 95% CI 0.64-0.88; p < 0.001):
![Updated follow-up for this Brazilian trial in 2025 [4] reported that there were 452 biochemical recurrence events at a median follow-up of 4.2 years. The results confirmed the previous finding of comparable biochemical recurrence rates between the arms (HR 1.05, 95% CI 0.97-1.13; p = 0.30). However, with 123 metastasis events and a median follow-up of 5.4 years for patients without metastasis, they found a clinically and statistically significant protective effect of extended pelvic lymph node dissection against metastasis (any metastasis: HR 0.82, 95% CI 0.71-0.93; p = 0.003; distant metastasis: HR 0.75, 95% CI 0.64-0.88; p < 0.001):](/images/com-doc-importer/263-aua-2026/aua-2026-role-of-lymph-node-dissection-at-the-time-of-radical-prostatectomy/image-4.jpg)
Dr. Esen then discussed staging PSMA PET/CT for prostate cancer. The 2026 EAU guidelines for unfavorable intermediate risk prostate cancer provide a weak recommendation for performing a PSMA PET/CT to increase the accuracy of staging compared to CT and bone scan. For high-risk localized disease, there is a strong recommendation for performing a PSMA PET/CT.
In work from Dr. Esen’s group,5 in 2021, they evaluated the accuracy of 68Ga-PSMA-11 PET/CT for lymph node metastasis detection in 96 patients undergoing radical prostatectomy and extended pelvic lymph node dissection, comparing the results of imaging to central pathology review. Among these 96 patients, 15 (15.6%) had lymph node metastasis. This study found that the per-patient sensitivity and specificity in the detection of lymph node metastasis >= 3 mm were 61.5% and 98.8%, respectively.
A study from the Martini-Klinik in 20256 assessed the diagnostic accuracy of PSMA PET/CT for primary lymph node staging before radical prostatectomy, noting that among 873 patients, 25% had lymph node invasion. In the overall cohort, the per-patient sensitivity, specificity, positive predictive value, negative predictive value, and accuracy calculated for lymph node invasion detection via PSMA PET/CT were 45.5%, 92.6%, 67.6%, 83.4%, and 80.8%, respectively. The median metastatic lymph node size in the group of 120 patients with false-negative PET/CT results was 2.5 mm. For metastatic lymph nodes ≥5 mm, the sensitivity and negative predictive value increased to 68.8% (+23.3%) and 95.4% (+12.0%), respectively.
Can a negative PSMA PET/CT avoid the need for pelvic lymph node dissection in newly diagnosed prostate cancer? To answer this question, in 2022, Stabile et al.7 performed a systematic review and meta-analysis of the available literature. There were 27 studies and 2,832 patients included in the analysis, with the following results: sensitivity, specificity, positive predictive value, and negative predictive value of PSMA PET/CT for lymph node invasion were 58%, 95%, 79%, and 87%. This study concluded that the high negative predictive value in men with a lower risk of lymph node invasion may be clinically useful to reduce the number of unnecessary pelvic lymph node dissection procedures performed. Conversely, in high-risk patients, a negative PSMA PET/CT cannot replace staging pelvic lymph node dissection.
Dr. Esen’s group recently assessed the performance of PSMA PET/CT in nodal staging of intermediate-risk prostate cancer and evaluated the effect of pelvic lymph node dissection on oncological outcomes of 308 intermediate-risk prostate cancer patients with a negative PSMA PET/CT.8 The sensitivity, specificity, positive predictive value, and negative predictive value of PSMA PET/CT on nodal staging were 53.3%, 95%, 47.1%, and 96.1%, respectively. The negative predictive value of PSMA PET/CT in patients with biopsy Grade Group 3 disease (96.3%) was similar to that of those with biopsy Grade Group 2 disease (95.6%). The median follow-up after propensity score matching was 20.7 months, and the 24-month biochemical recurrence-free survival rates were 83.7% and 86.9% in the pelvic lymph node dissection group and radical prostatectomy-only groups, respectively (p = 0.078):

Thus, Dr. Essen notes that pelvic lymph node dissection may be omitted in PSMA PET/CT-negative intermediate-risk prostate cancer, although prospective validation is warranted.
Integrating PSMA PET with nomograms in intermediate risk cases could optimize patient selection for extended pelvic lymph node dissection, potentially reducing unnecessary surgeries without increasing the risk of missed lymph node invasion cases. Preoperative staging with PSMA PET may play both exclusive and inclusive roles in the intermediate-risk setting. If PSMA PET shows N0, it may exclude candidates from extended pelvic lymph node dissection. Additionally, when combined with nomograms, it may help select candidates for extended pelvic lymph node dissection among patients who show a high risk of lymph node invasion according to risk calculators.
It is important to emphasize that lymphadenectomy may cause harm. Collectively, the literature suggests that lower limb lymphedema following radical prostatectomy occurs in 0-14% of patients who undergo a pelvic lymph node dissection, which compares to 0-9% for those undergoing pelvic lymph node radiotherapy. For patients who are undergoing pelvic lymph node dissection and salvage pelvic lymph node radiotherapy, these rates increase to 19-29%, with 2-22% also developing genital lymphedema. Additionally, there is a 6-10 times increased risk of deep venous thrombosis and pulmonary embolism. Dr. Esen notes that the lack of a uniform definition and standardized diagnostic criteria for lower limb and genital lymphedema hampers the accurate estimation of their true prevalence.
What do the experts say about pelvic lymph node dissection for prostate cancer? The following statements are from members of the EAU guidelines:9
- PSMA PET/CT is characterized by a high negative predictive value when the risk of lymph node invasion is low. Therefore, extended pelvic lymph node dissection can be avoided when the risk is low, and PSMA-PET/CT is negative
- Surgeons may consider selected patients with high-risk, aggressive disease, who might harbour micro-metastatic lymph node invasion, for a staging extended pelvic lymph node dissection
- The change of recommendations in 2024 was in part driven by the decision to recommend PSMA-PET for staging assessment of patients prior to treatment. PSMA-PET/CT is highly specific but with a negative predictive value of approximately 80%, where most of the missed metastases are low volume (number of affected nodes, size of nodal deposits). However, its ability to identify additional lymph node deposits beyond conventional imaging reduces the gap between imaging and pathological staging to fundamentally alter the risk-benefit ratio
Dr. Esen concluded his presentation discussing the role of lymph node dissection at the time of radical prostatectomy with the following take-home points:
- For intermediate risk disease, pelvic lymph node dissection may safely be omitted if PSMA PET is negative for lymphovascular invasion, as missed lymph nodes are small and may also be missed in extended pelvic lymph node dissections
- In Grade Group 3 disease, nomograms can be of additional use
- For high-risk disease, the decision is individual and should be discussed with the patient at length, including the possibility that an adjuvant/salvage pelvic radiotherapy may increase side effects
- If pelvic lymph node dissection is to be performed, then it should be in an extended fashion
Presented by: Tarik Esen, MD, Koç University, Istanbul, Turkey
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Fossati N, Willemse PPM, van den Broeck T, et al. The benefits and harms of different extents of lymph node dissection during radical prostatectomy for prostate cancer: A systematic review. Eur Urol. 2017 Jul;72(1):84-109.
- Lestingi JFP, Guglielmetti G, Trinh QD, et al. Extended versus limited pelvic lymph node dissection during radical prostatectomy for intermediate- and high-risk prostate cancer: Early oncological outcomes from a randomized phase 3 trial. Eur Urol. 2021 May;79(5):595-604.
- Touijer KA, Sjoberg DD, Benfante N, et al. Limited versus extended pelvic lymph node dissection for prostate cancer: A randomized clinical trial. Eur Urol Oncol. 2021 Aug;4(4):532-539.
- Touijer KA, Vertosick EA, Sjoberg DD, et al. Pelvic lymph node dissection in prostate cancer: Update from a randomized clinical trial of limited versus extended dissection. Eur Urol. 2025 Feb;87(2):253-260.
- Esen T, Falay O, Tarim K, et al. 68Ga-PSMA-11 Positron Emission Tomography/Computed Tomography for Primary Lymph Node Staging Before Radical Prostatectomy: Central Review of Imaging and Comparison with Histopathology of Extended Lympadenectomy. Eur Urol Focus. 2021 Mar;7(2):288-293.
- Incesu RB, Preisser F, Pompe RS, et al. Diagnostic accuracy of prostate-specific membrane antigen positron emission tomography/computed tomography for primary lymph node staging before radical prostatectomy. Eur Urol Focus. 2025 Jul;11(4):582-587.
- Stabile A, Pellegrino A, Mazzone E, et al. Can negative positron emission tomography/computed tomography avoid the need for pelvic lymph node dissection in newly diagnosed prostate cancer patients? A systematic review and meta-analysis with backup histology as reference standard. Eur Urol Oncol. 2022 Feb;5(1):1-17.
- Esen B, Seymen H, Armutlu A, et al. Impact of pelvic lymph node dissection on early oncological outcomes in intermediate-risk prostate cancer patients with node-negative PSMA PET. Prostate. 2025 Jun;85(8):777-783.
- Roberts MJ, Gandaglia G, Oprea-Lager DE, et al. Pelvic lymph node dissection in prostate cancer: Evidence and implications. Eur Urol. 2025 Jun;87(6):619-621.