(UroToday.com) The American Urological Association's 2026 Annual Meeting, in Washington D.C., was host to the AUA-IBCG Bladder Cancer Forum. Drs. Paolo Gontero, Jeffrey Ross, Badrinath Konety and Maurizio Brausi Debated Next Generation Markers – Is it Time to Let Go of our Old Friends?
Dr. Konety began by reviewing historical trends in the diagnostic evaluation of bladder cancer. Over time, the use of cross-sectional imaging with CT and MRI has steadily increased, while utilization of older modalities such as intravenous pyelography declined significantly. Cytologic analysis rates remained relatively stable throughout the study period, reflecting the continued role of urine cytology as part of the diagnostic workup despite evolving imaging technologies.
He subsequently reviewed trends in urinary marker utilization over time, demonstrating increasing adoption of urinary marker testing alongside cytology in bladder cancer evaluation. Importantly, he highlighted data suggesting that incorporation of urinary marker testing was associated with improved cancer-specific mortality outcomes.1 However, despite these potential benefits, adoption in routine clinical practice remains limited. He emphasized that even highly performant biomarkers continue to face significant barriers to widespread implementation, with real-world data showing that urologists still underutilize urinary biomarkers despite evidence suggesting a meaningful reduction in cancer-specific mortality.
To illustrate the potential role of novel urinary biomarkers, Dr. Konety presented the case of a 79-year-old patient with a history of HTN who initially presented with hematuria and LUTS eight years earlier. Workup revealed bladder stones and CIS, and the patient subsequently underwent BCG plus maintenance therapy for three years. Following positive cytology and UroVysion testing, the patient received intravesical gemcitabine/docetaxel, later developing recurrent CIS treated with nadofaragene firadenovec (Adstiladrin), achieving a complete response for three years.
Despite negative bladder biopsies, the patient later developed persistent atypical cytology and positive UroVysion testing, with a positive right ureteral wash raising concern for upper tract involvement. Using this case, the discussion focused on several clinically relevant questions, including whether surveillance strategies could be improved with novel urinary markers, how newer assays compare with conventional cytology and FISH, whether these biomarkers may improve diagnostic triage, and the evolving role of novel markers in UTUC detection and surveillance.
Next Generation Markers are Ready for Prime TimeDr Brausi began by discussing the limitations of the current standard monitoring tools used in bladder cancer surveillance, particularly cystoscopy and urine cytology. Cystoscopy was noted to have a sensitivity of approximately 70–80% for high-grade disease with specificity around 70%, but remains an invasive and often uncomfortable procedure requiring significant urologic expertise. In contrast, urine cytology offers a non-invasive alternative with high specificity ranging from 90–95%, although sensitivity for high-grade disease remains lower at approximately 50–60%. Additionally, cytology interpretation is operator-dependent and requires specialized cytopathology expertise. Together, these limitations highlight the ongoing unmet need for more accurate, accessible, and patient-friendly biomarker-based surveillance strategies.
Dr. Brausi subsequently reviewed the emerging role of multiplex urinary marker panels in bladder cancer (figure below) detection and surveillance. Unlike single-marker assays such as cytology or NMP22, multiplex platforms simultaneously evaluate multiple bladder cancer-associated biomarkers, potentially improving diagnostic accuracy while reducing false positives related to benign inflammatory conditions such as stones or urinary tract infections.
He highlighted that several multiplex assays have demonstrated sensitivities exceeding 90% for high-grade tumors, with specificities ranging from 91–100%. Potential clinical applications include initial diagnosis, recurrence monitoring, and prediction of treatment response, particularly in patients receiving intravesical therapies such as BCG.
He additionally reviewed several next-generation urinary biomarkers currently being developed and incorporated into clinical practice across different disease settings. For diagnosis in patients presenting with hematuria, assays such as AssureMDx, CX Bladder, EpiCheck, and Galeas were highlighted, with reported sensitivities ranging from 90–98% and negative predictive values approaching 98–99%.
In the surveillance setting, newer markers including Xpert, CX Bladder, ADXBladder, utDNA-based assays, and EpiCheck are being explored as strategies to reduce the frequency of surveillance cystoscopy while maintaining diagnostic accuracy. Emerging biomarkers predictive of treatment response (shown below) were also discussed, including Oncuria for chemotherapy response prediction, urinary ctDNA assays in the setting of chemo-BCG, CyPRIT for BCG response assessment, and artificial intelligence-based platforms aimed at improving prediction of therapeutic outcomes.

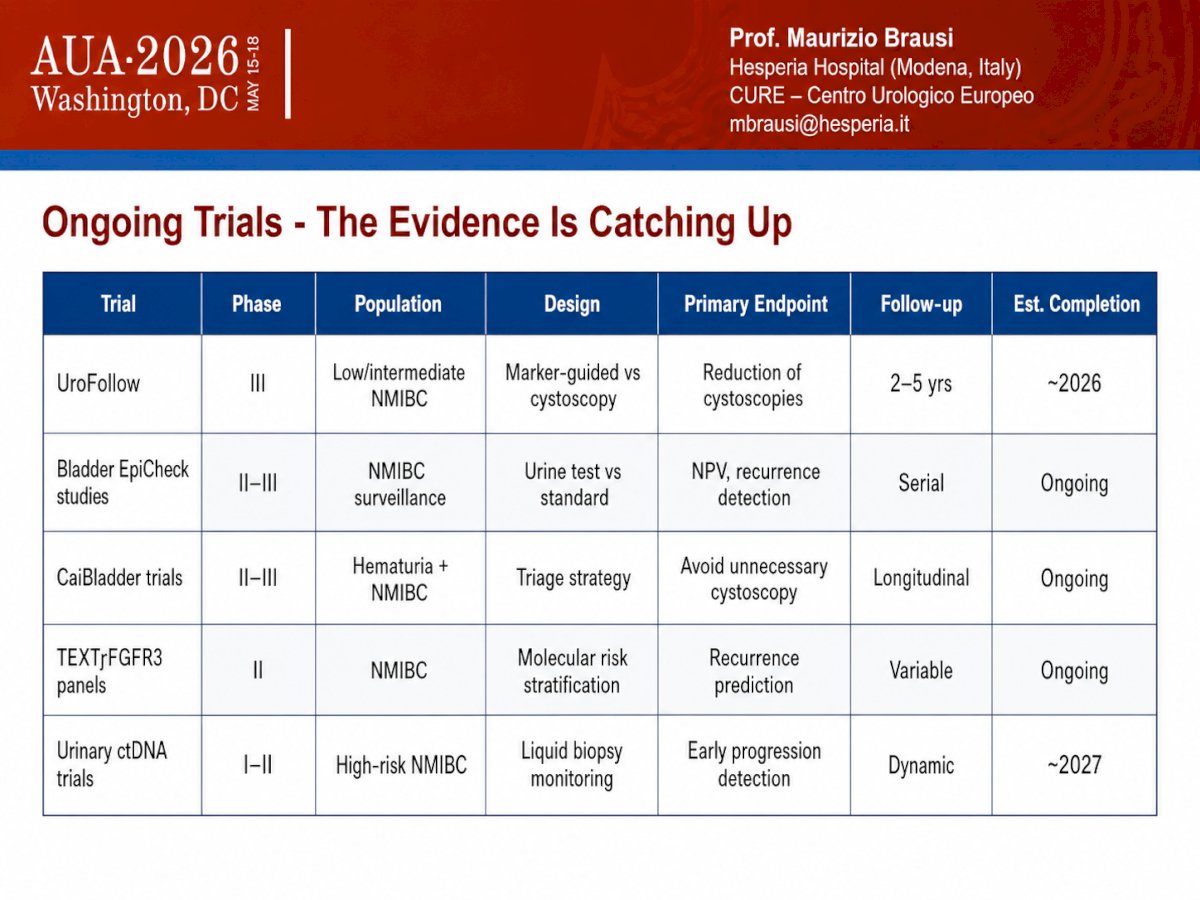
Dr. Brausi summarzed several ongoing clinical trials (Table below) evaluating the integration of urinary biomarkers into bladder cancer diagnosis and surveillance strategies. These include the phase III UroFollow trial in low- and intermediate-risk NMIBC comparing marker-guided surveillance versus cystoscopy with the goal of reducing cystoscopic procedures, as well as multiple phase II–III studies evaluating EpiCheck and CxBladder in NMIBC surveillance and hematuria triage settings. Additional ongoing efforts include FGFR3-based molecular risk stratification panels aimed at recurrence prediction and urinary ctDNA trials focused on early progression detection in high-risk NMIBC. Collectively, these studies reflect the growing momentum toward biomarker-driven bladder cancer management, with evidence increasingly “catching up” to support broader clinical implementation.
Lastly, Dr. Brausi highlighted a recent systematic review and meta-analysis evaluating Bladder EpiCheck in patients with upper tract urothelial carcinoma (UTUC). Across 334 patients, the assay demonstrated a sensitivity of 85%, specificity of 93%, PPV of 74%, and NPV of 84%, with improved performance for high-grade compared with low-grade tumors.2 He emphasized that these findings suggest Bladder EpiCheck may help reduce or postpone invasive procedures such as ureteroscopy, potentially lowering complication risk while improving patient quality of life.
He also reviewed comparative data evaluating Xpert versus FISH and cytology in UTUC, noting excellent sensitivity for high-grade disease, while acknowledging that urinary markers continue to have limited utility in low-grade tumors.2
Dr. Brausi concluded his presentation with the following key takeaways:
- No genetic or urinary biomarker is currently ready to entirely replace standard tools such as cystoscopy and cytology in the routine management of bladder cancer.
- However, sufficient evidence now supports the use of selected urinary biomarkers to reduce or replace cystoscopy in appropriate clinical settings, particularly among low- and intermediate-risk patients, and in selected high-risk surveillance populations. Biomarkers highlighted included EpiCheck, Xpert Bladder Cancer Monitor, and CxBladder.
- Alternating cystoscopy with urinary biomarkers may represent a smart and practical integration strategy within surveillance protocols.
- Use of these biomarkers has the potential to improve quality of life while simultaneously reducing healthcare costs.
- Next-generation urinary markers are becoming increasingly important, particularly in elderly or frail patients, those with significant comorbidities, or individuals receiving anticoagulation therapy, where surveillance de-intensification may be especially valuable.
- While ongoing phase III trials are still awaited to further validate the currently available data, the existing evidence supporting these technologies is increasingly convincing.
- He concluded with a direct call to action, emphasizing: “It’s time to adopt them.”
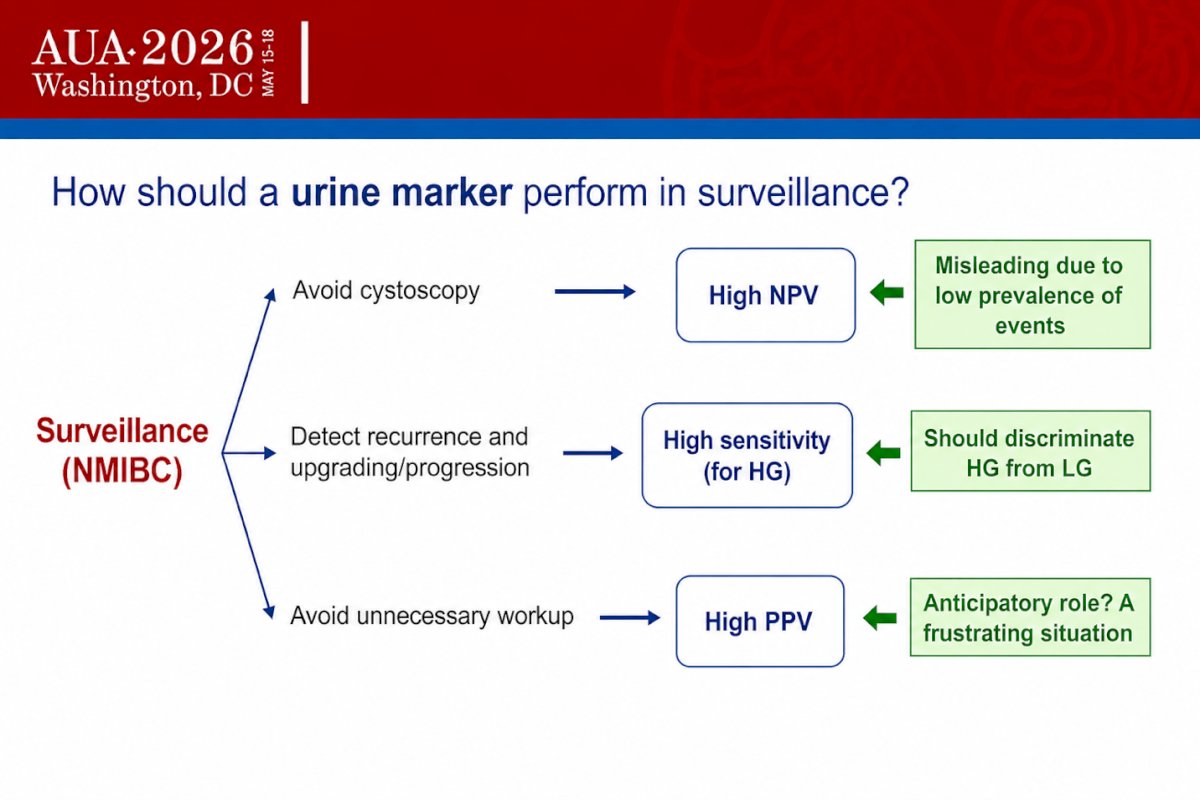
Dr. Paolo Gontero began by discussing the ideal performance characteristics of urinary markers in the surveillance setting for NMIBC. He emphasized that one of the most important features is a high negative predictive value (NPV), as this could help safely reduce the frequency of cystoscopy. However, he cautioned that an NPV of 90% may still be insufficient in certain clinical scenarios, particularly in patients at risk for high-grade recurrence.
He further noted that urinary markers used for surveillance must demonstrate very high sensitivity, especially for high-grade tumors, with the ability to discriminate high-grade from low-grade recurrence. In addition, high positive predictive value (PPV) remains important to minimize unnecessary diagnostic workup and avoid frustrating clinical situations created by false-positive results.
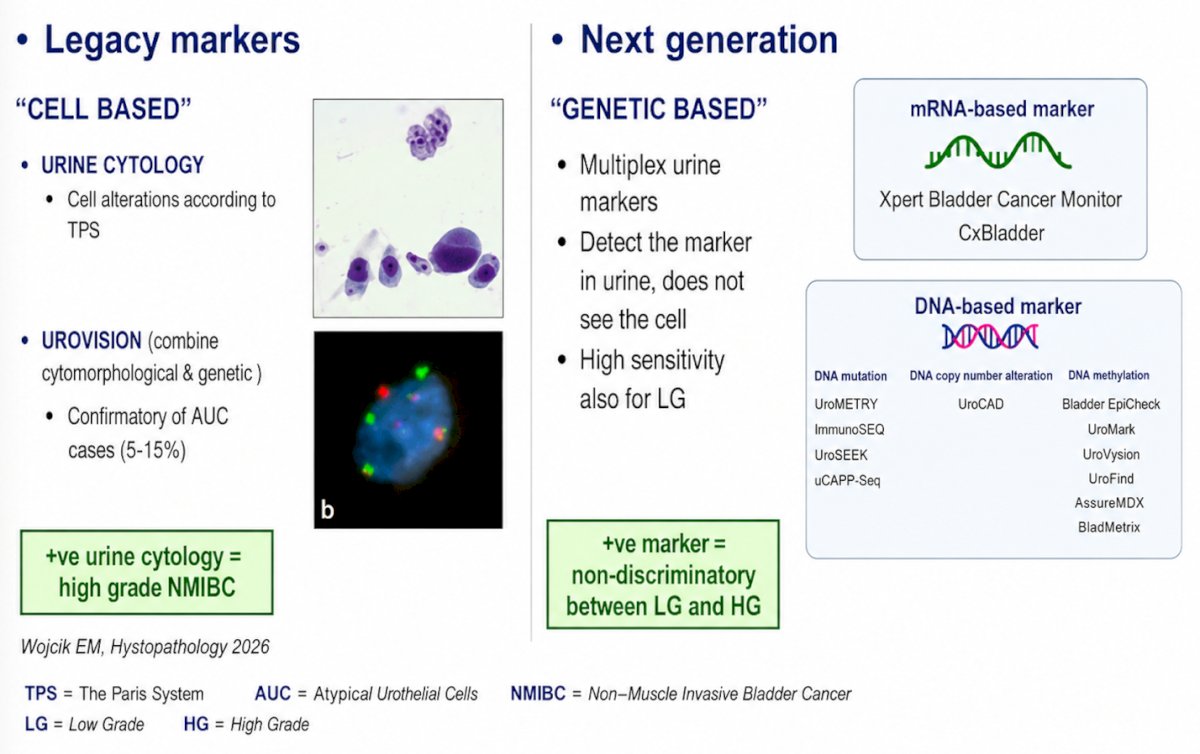
He went on to discuss the evolution from “legacy” cell-based urinary markers toward next-generation genetic-based assays. Legacy markers, including urine cytology and UroVysion, rely on cytomorphologic evaluation and remain particularly useful for the detection of high-grade disease. In fact, he emphasized that a positive urine cytology is highly associated with high-grade NMIBC (as shown in the figure below)
By contrast, next-generation urinary markers are largely genetic-based assays that detect molecular alterations in urine rather than directly evaluating cells. These include multiplex mRNA- and DNA-based platforms such as Xpert Bladder Cancer Monitor, CxBladder, UroMety, UroCAD, Bladder EpiCheck, and others. While these assays generally demonstrate higher sensitivity, including for low-grade tumors, he noted an important limitation: many next-generation markers are less able to discriminate between low-grade and high-grade recurrence.
He subsequently reviewed the performance characteristics of several next-generation multiplex urinary markers, highlighting their generally high sensitivity for high-grade disease. Xpert Bladder Cancer Monitor and EpiCheck demonstrated overall sensitivities ranging from approximately 52–91% and 62–90%, respectively, with sensitivities for high-grade tumors approaching 79–100% and 78–95%. CxBladder also showed strong performance, with reported sensitivities of 93% overall and 95% for high-grade disease.
However, despite these encouraging results, he emphasized several important limitations of next-generation assays, including variability in reproducibility across studies, uncertainty regarding their ability to reliably identify tumors at highest risk for progression, and lower-than-expected sensitivity for certain platforms, such as utDNA in high-grade disease. He also noted that while these markers perform well for detection, they still provide limited information regarding tumor biology and grade progression.
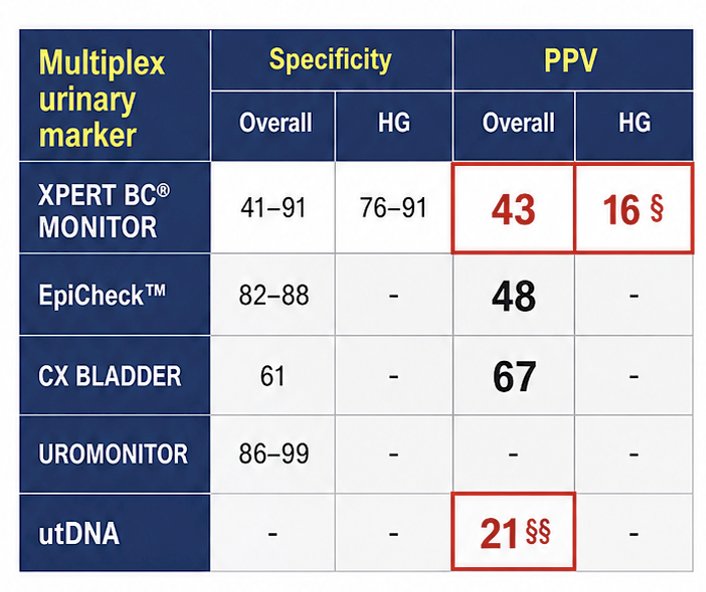
Moreover, Dr. Gontero emphasized that specificity and positive predictive value (PPV) remain critical considerations when evaluating next-generation urinary markers. While many assays demonstrate strong sensitivity for high-grade disease, PPV continues to represent an important limitation in the surveillance setting. In contrast, legacy markers such as urine cytology maintain relatively high specificity (~89%) and PPV approaching 79%. Among next-generation platforms, Xpert Bladder Cancer Monitor demonstrated an overall PPV of approximately 43%, whereas utDNA assays showed PPV values as low as 21% in some series. He further highlighted recent randomized data in high-risk surveillance populations where PPV dropped to only 16% for certain assays. According to Dr. Gontero, these findings raise important concerns regarding excessive downstream testing and the “anticipatory effect” generated by persistently positive biomarkers in patients without clinically evident recurrence.
Dr. Gontero also highlighted a systematic review including 11 studies published between 2017 and 2024 evaluating artificial intelligence (AI)-assisted urinary cytology. Across these series, both sensitivity and specificity were generally higher with AI-supported approaches compared with traditional cytology, with some studies reporting near-perfect diagnostic accuracy.
Importantly, AI-assisted cytology significantly improved sensitivity versus conventional cytology in certain studies, reaching 93% compared with 62% using standard assessment alone. He also noted that sensitivity improved substantially when cytology was interpreted by expert genitourinary pathologists within a multidisciplinary discussion framework, exceeding 60% in several reports. Overall, AI-guided urine cytology appeared to outperform expert pathologist interpretation while also reducing inter-operator variability and diagnostic workload.3,4
Dr. Gontero concluded his presentation with the following key takeaways:
- The high sensitivity of next-generation urinary markers carries important inherent limitations.
- Many next-generation assays lack the ability to reliably discriminate high-grade disease, limiting their utility for identifying progression.
- These markers may have limited value during follow-up of low-grade tumors and active surveillance populations.
- Low PPV and false-positive results with next-generation assays can drive excessive downstream testing and work against efforts to safely de-intensify surveillance strategies.
- He also cautioned about the potential “anticipatory effect” of persistently positive biomarkers outside selected populations, such as patients with BCG-unresponsive disease.
- Despite increasing interest in novel assays, legacy urinary markers such as urine cytology remain highly relevant and are “far from dead.”
- Urine cytology retains a unique ability to specifically identify high-grade recurrence.
- Emerging technologies, including AI-assisted cytology, may help overcome operator dependence and improve diagnostic accuracy.
- Ultimately, legacy and next-generation markers should be viewed as complementary tools, with integration of both approaches potentially allowing safer surveillance de-intensification while minimizing overdiagnosis and overtreatment.
- Paolo Gontero, MD, Professor, Chairman Department of Urology, Molinette Hospital, University School of Medicine, Torino, Italy
- Badrinath Konety, MD, MBA, Professor at the University of Minnesota, Director of the Institute for Prostate and Urologic Cancers. He is also Associate Director, Clinical Affairs & Clinical Research, Masonic Cancer Center (MCC), MN, United States.
- Maurizio Brausi, MD, Dept. of Urology, AUSL Modena, Italy.
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference:
- Narayan VM, Adejoro O, Schwartz I, Ziegelmann M, Elliott S, Konety BR. The Prevalence and Impact of Urinary Marker Testing in Patients with Bladder Cancer. J Urol. 2018 Jan;199(1):74-80. doi: 10.1016/j.juro.2017.08.097. Epub 2017 Aug 30. PMID: 28859894.
- Artero Fullana S, Caño Velasco J, Lafuente Puentedura A, Polanco Pujol L, Bataller Monfort V, Moralejo Gárate M, Subiela JD, Gallioli A, Moschini M, Pichler R, Del Giudice F, Marcq G, Teoh J, Soria F, Mertens L, Krajewski W, Laukhtina E, Mori K, Pradere B, Afferi L, Tully KH, Albisinni S, Abu Ghanem Y, d'Andrea D, Mari A, Albers Acosta E, Contieri R, Cimadamore A, Grobet-Jeandin E, Gómez Rivas J, Hernández Fernández C; en representación del Grupo de Trabajo de Carcinoma Urotelial de la Sección de Jóvenes Urólogos Académicos - Asociación Europea de Urología (EAU-YAU). Diagnostic accuracy of Bladder EpiCheck for upper tract urothelial carcinoma: A meta-analysis. Actas Urol Esp (Engl Ed). 2025 May;49(4):501720. English, Spanish. doi: 10.1016/j.acuroe.2025.501720. Epub 2025 Feb 13. PMID: 39955057.
- Tsuji K, Kaneko M, Harada Y, Fujihara A, Ueno K, Nakanishi M, Konishi E, Takamatsu T, Horiguchi G, Teramukai S, Ito-Ihara T, Ukimura O. A Fully Automated Artificial Intelligence System to Assist Pathologists' Diagnosis to Predict Histologically High-grade Urothelial Carcinoma from Digitized Urine Cytology Slides Using Deep Learning. Eur Urol Oncol. 2024 Apr;7(2):258-265. doi: 10.1016/j.euo.2023.11.009. Epub 2023 Dec 7. PMID: 38065702.
- Nabiyouni F, Chiou PZ. Enhancing urine cytopathology with artificial intelligence: a systematic review. Am J Clin Pathol. 2026 Jan 5;165(2):aqaf135. doi: 10.1093/ajcp/aqaf135. PMID: 41643205.