(UroToday.com) At the 2026 American Urological Association (AUA) Annual Meeting in Washington, DC, the AUA–International Bladder Cancer Group (IBCG) Bladder Cancer Forum hosted a practical debate addressing one of the most relevant contemporary questions in non–muscle-invasive bladder cancer (NMIBC): what should be considered the preferred first-line bladder-preserving therapy for patients with BCG-unresponsive high-risk disease who are unwilling or unfit to undergo radical cystectomy? The discussion reflected the rapidly expanding therapeutic landscape, which now includes FDA-approved agents such as pembrolizumab, nadofaragene firadenovec, nogapendekin alfa inbakicept plus BCG, and Inlexzo (Gem-iDRS), alongside the widely adopted sequential intravesical combination of gemcitabine and docetaxel. Following a case presentation by Dr. Vignesh Packiam, Dr. Amanda Myers argued that gemcitabine/docetaxel has become the de facto first-line option, whereas Dr. Bogdana Schmidt contended that no single therapy should be considered the universal default, and that treatment selection should instead reflect a deliberate, individualized sequencing strategy.
Dr. Packiam opened the debate with a representative clinical case of a 66-year-old man who presented with gross hematuria and had a 20 pack-year smoking history, hypertension, hyperlipidemia, and type 2 diabetes mellitus. CT urography demonstrated a 4 cm left lateral wall bladder tumor with no upper tract lesions, lymphadenopathy, or metastatic disease. Initial transurethral resection of bladder tumor (TURBT) revealed high-grade T1 urothelial carcinoma on the left lateral wall and concomitant carcinoma in situ (CIS) identified on blue-light cystoscopy at the bladder dome. Repeat TURBT was benign. The patient subsequently received full-dose induction BCG followed by one-third dose maintenance at 3 and 6 months. Surveillance cystoscopy demonstrated multifocal subcentimeter papillary recurrences and an erythematous trigonal lesion. Repeat CT urography remained negative, and TURBT confirmed recurrent high-grade Ta disease with concomitant CIS, meeting criteria for BCG-unresponsive high-risk NMIBC.
Dr. Packiam used this case to frame the central question of the session: among the expanding array of bladder-preserving options, which treatment should be offered first to a patient who strongly wishes to avoid radical cystectomy?
Dr. Myers argued that sequential intravesical gemcitabine/docetaxel has effectively become the de facto first-line therapy for many patients with BCG-unresponsive disease because it combines durable efficacy, favorable tolerability, low cost, and broad accessibility. She began by emphasizing that no bladder-sparing therapy has demonstrated clear superiority in head-to-head trials. Accordingly, treatment selection should be guided not only by efficacy, but also by safety, treatment burden, cost, and availability.
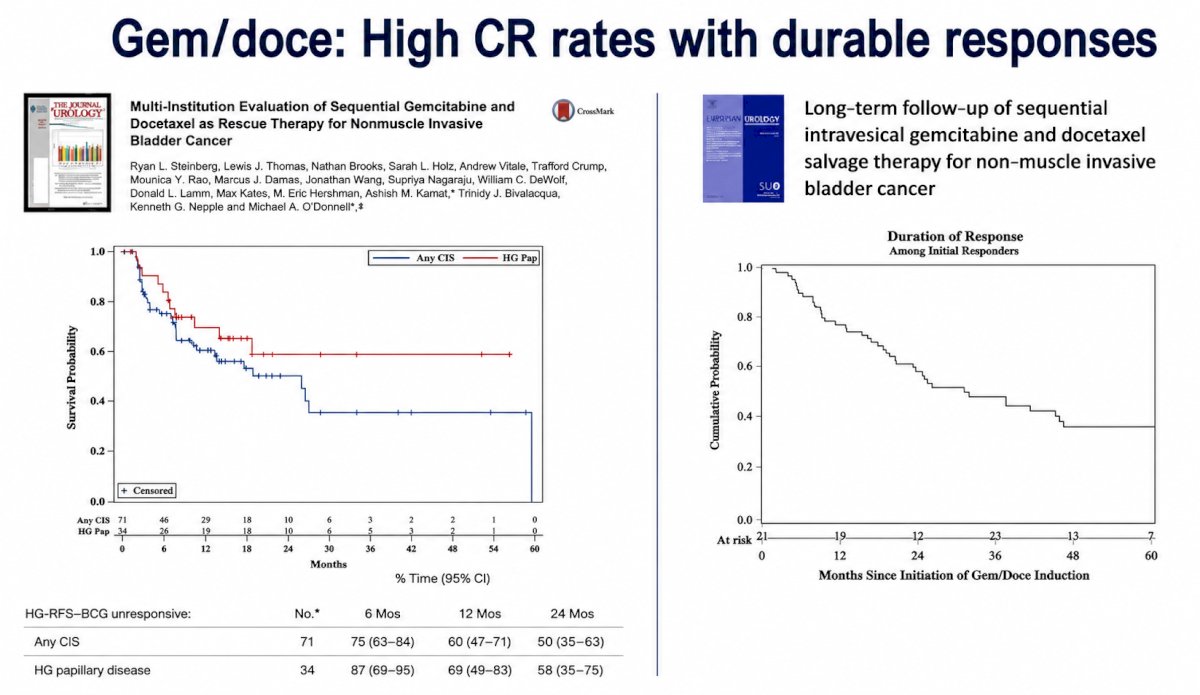
She reviewed the original University of Iowa experience reported by Ryan Steinberg and colleagues. Among 71 patients with BCG-unresponsive CIS, high-grade recurrence-free survival was 75% at 6 months, 60% at 12 months, and 50% at 24 months. In patients with high-grade papillary-only disease, corresponding rates were 87%, 69%, and 58%, respectively. Long-term follow-up demonstrated a median duration of response of approximately 24 months.1,2 She also highlighted a prospective cohort from the Netherlands that confirmed these findings, with high-grade disease-free survival in patients with BCG-unresponsive CIS of 75% at 6 months, 69% at 12 months, 69% at 18 months, and 46% at 24 months.3
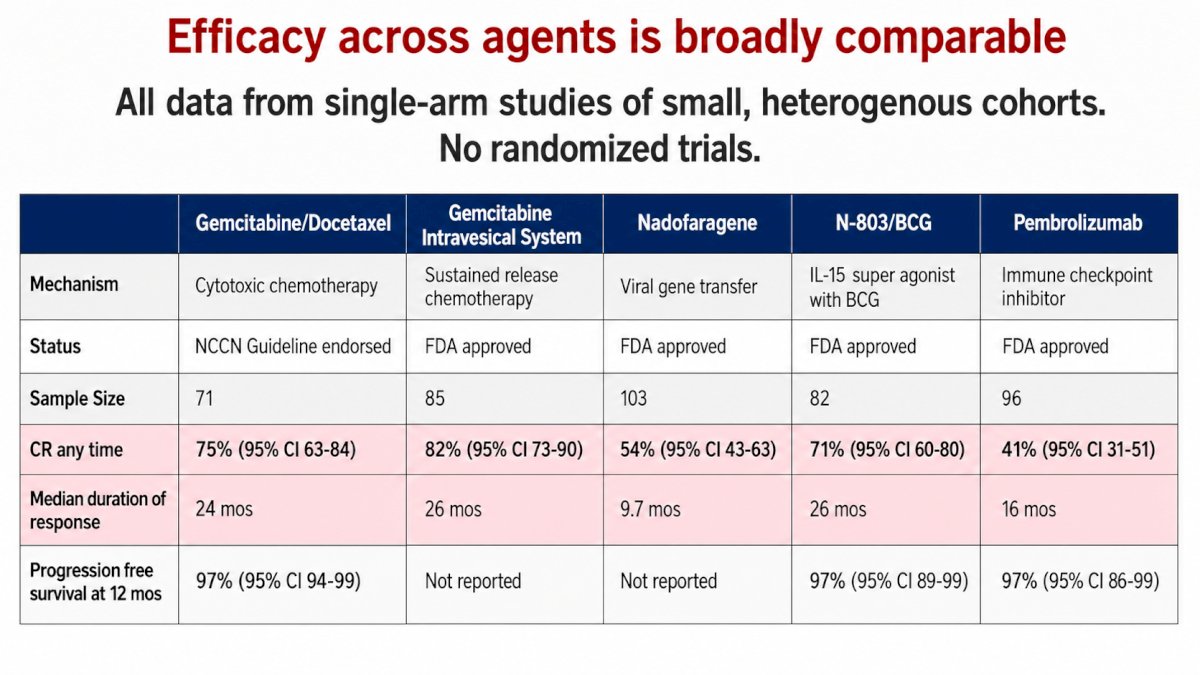
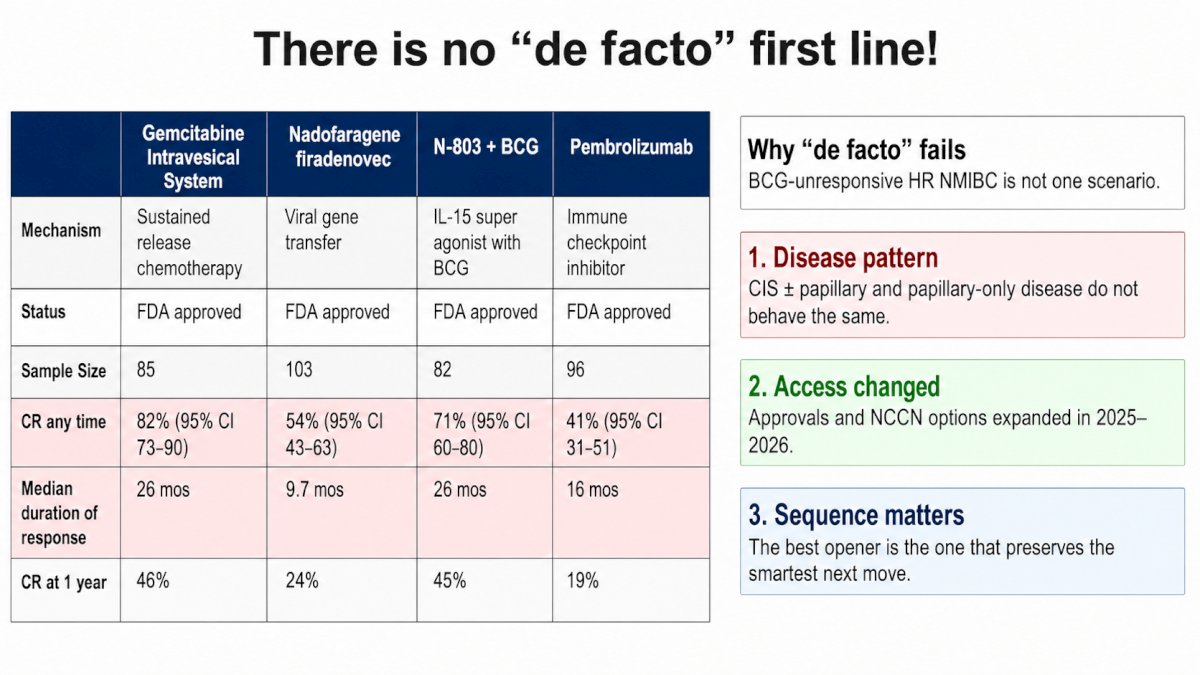
Dr. Myers then compared gemcitabine/docetaxel with other available therapies using cross-trial data. Gemcitabine/docetaxel achieved an overall complete response rate of approximately 75% with a median duration of response of 24 months. These outcomes compared favorably with those reported for nadofaragene firadenovec (54% complete response, median duration of response 9.7 months), Nogapendekin alfa inbakicept plus BCG (71% complete response, median duration of response 26 months), and pembrolizumab (41% complete response, median duration of response 16 months). She also highlighted emerging data with intravesical gemcitabine delivery systems, which have reported complete response rates approaching 82% and median duration of response of approximately 26 months.
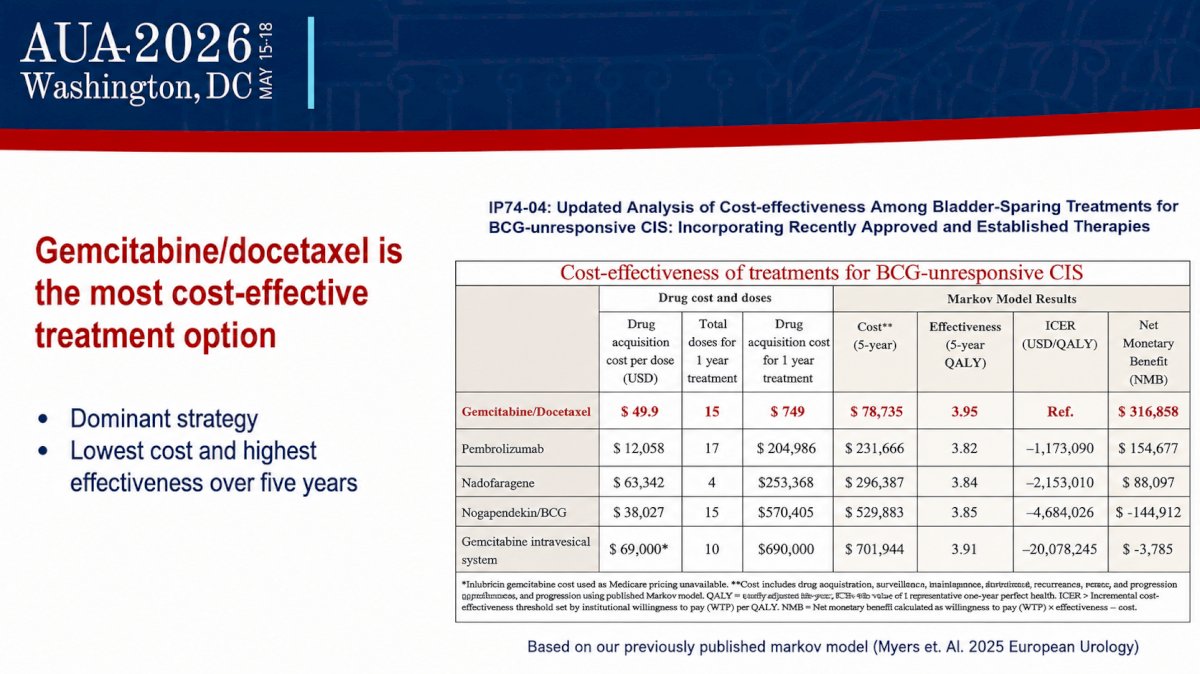
A major component of Dr. Myers’ argument centered on tolerability and value. Sequential gemcitabine/docetaxel is associated with low rates of treatment discontinuation due to adverse events (3.3%) and treatment delays due to toxicity (9%). In addition, a 2025 cost-effectiveness analysis found gemcitabine/docetaxel to be the dominant strategy, yielding the lowest overall cost and the highest estimated 5-year effectiveness at 3.95 quality-adjusted life years.
She also emphasized its remarkable global uptake, with routine use reported throughout North America, Europe, the Middle East, Asia, and Australia. Her conclusion was that, in the absence of definitive comparative trials, gemcitabine/docetaxel has emerged as the practical first choice for many clinicians because it offers durable disease control, excellent tolerability, low cost, and universal availability.
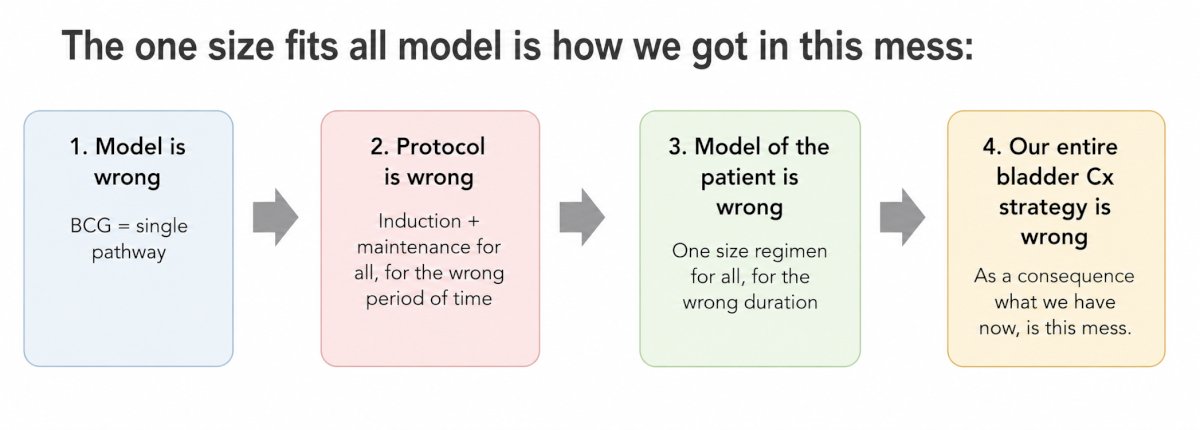
Dr. Schmidt presented the opposing viewpoint, arguing that the field has moved beyond a one-size-fits-all approach and that no single therapy should be considered the universal first-line standard. Her central message was summarized by the title of her presentation: “Dealer’s Choice: Go BIG or Go HOME!” She emphasized that treatment selection in BCG-unresponsive NMIBC should be individualized according to tumor characteristics, patient priorities, evidence quality, treatment burden, and long-term sequencing considerations.
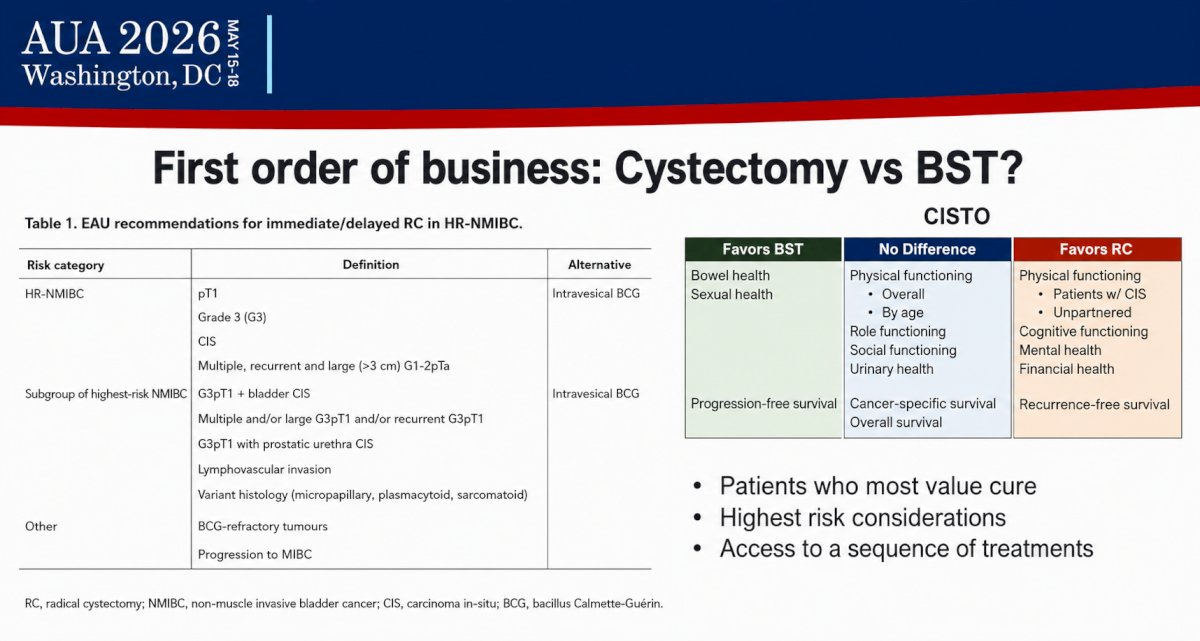
Dr. Schmidt began by reminding the audience that radical cystectomy remains the oncologic benchmark and should continue to be discussed with all appropriate candidates, particularly those with highest risk features such as persistent T1 disease, lymphovascular invasion, variant histology, or rapid recurrence. She noted that while bladder-sparing approaches may preserve urinary and sexual function, the decision to defer cystectomy must be made within the context of careful counseling regarding oncologic risk.
She then reviewed the currently available FDA-approved therapies and emphasized that each offers distinct advantages and limitations. Pembrolizumab provides a systemic option with durable responses in a subset of patients but requires intravenous administration and carries immune-related toxicity. Nadofaragene firadenovec offers quarterly intravesical dosing with a relatively low treatment burden. Nogapendekin alfa inbakicept plus BCG provides another effective intravesical immunotherapy-based approach. Inlexzo and other gemcitabine delivery platforms offer promising durability with infrequent dosing schedules. In her view, the diversity of mechanisms and treatment schedules argues against selecting one regimen as the default for all patients.
A central theme of Dr. Schmidt’s presentation was evidence hierarchy. She acknowledged that gemcitabine/docetaxel is a credible and highly useful regimen but emphasized that most supporting data are retrospective and therefore subject to selection bias, heterogeneous surveillance schedules, and non-standardized maintenance protocols. In contrast, FDA-approved agents were evaluated in prospective multicenter registration studies with predefined eligibility criteria, protocolized assessments, prospective adverse event collection, and formal regulatory review. She argued that when comparing non-randomized strategies, prospective registration-quality evidence should generally be weighted more heavily than retrospective institutional series.
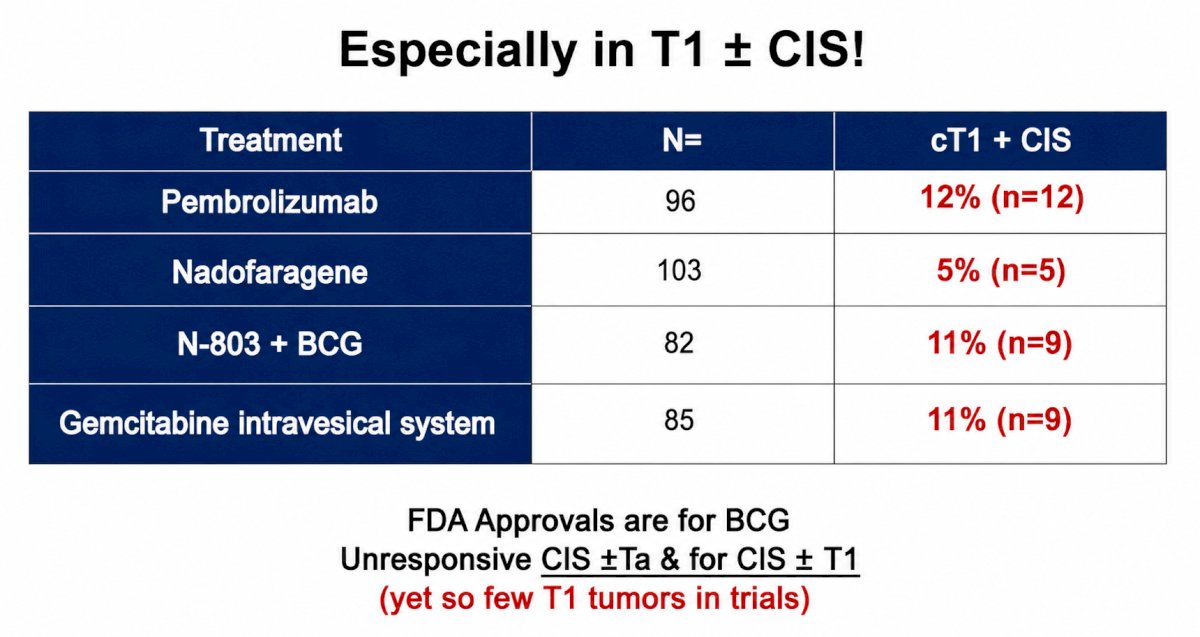
Dr. Schmidt also emphasized that trial populations differ substantially, particularly with respect to the representation of patients with T1 disease and concomitant CIS. She noted that only a small minority of patients in pivotal registration studies had cT1 ± CIS disease, limiting the generalizability of cross-trial comparisons to this highest-risk subgroup.
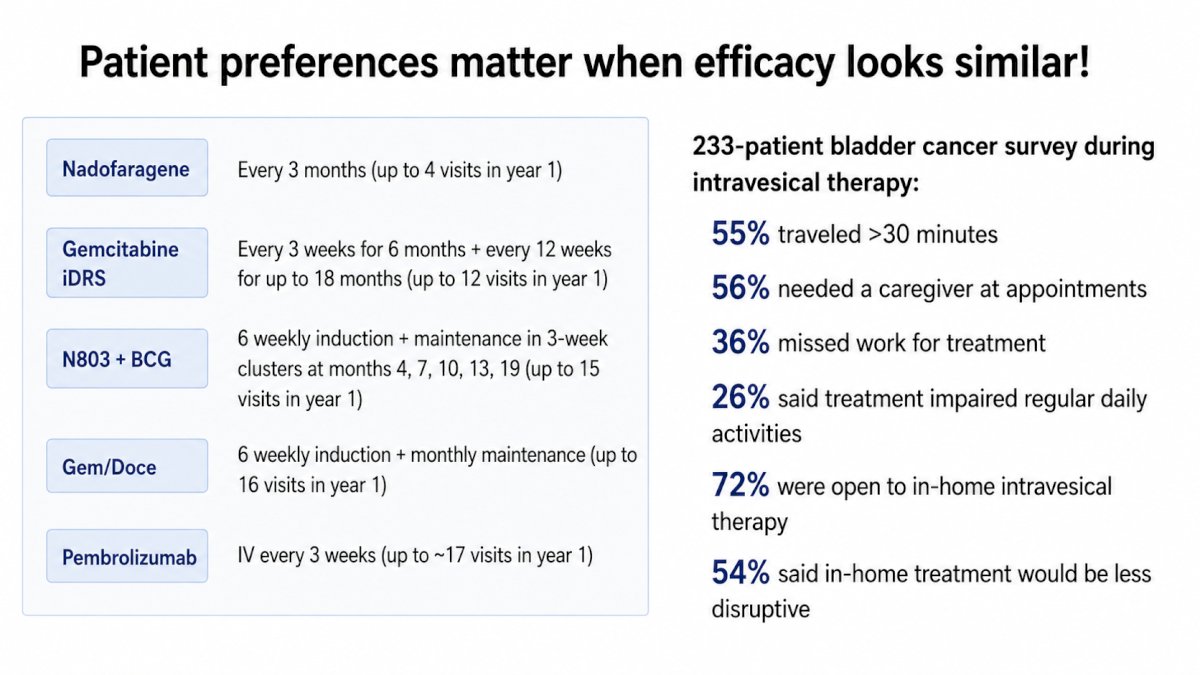
Another important aspect of her argument was treatment burden. She reviewed patient survey data demonstrating that more than half of patients travel over 30 minutes for treatment, more than half require caregiver support, over one-third miss work, and approximately one-quarter report disruption of daily activities. Given that many available therapies offer broadly comparable efficacy, she argued that convenience, frequency of visits, and impact on quality of life should play a central role in decision-making. Notably, a large majority of patients expressed interest in home-based intravesical treatment options.
Dr. Schmidt proposed a practical framework for therapy selection: match the disease phenotype (CIS versus papillary-only disease), preserve future treatment options by sequencing therapies with different mechanisms of action, identify the inflection point at which cystectomy should no longer be deferred, and optimize the entire treatment sequence rather than focusing narrowly on the first agent chosen.
She concluded by highlighting emerging biomarker-based strategies—including genomic profiling, transcriptomic classifiers, artificial intelligence–based pathology, and immune microenvironment characterization—that may eventually enable more precise treatment selection.
Taken together, this debate highlighted two complementary perspectives. Dr. Myers argued that gemcitabine/docetaxel has become the de facto first-line therapy because it provides durable efficacy, excellent tolerability, low cost, and global accessibility. Dr. Schmidt countered that no therapy has ‘earned the right’ to be considered the universal standard and that the best first-line treatment is the one that fits the patient’s disease biology, preferences, treatment burden, and anticipated salvage strategy.
The discussion underscored the remarkable evolution of the BCG-unresponsive NMIBC treatment landscape. Clinicians now have multiple effective bladder-preserving therapies with distinct mechanisms of action and treatment schedules. Rather than applying a uniform approach, treatment selection is increasingly centered on individualized sequencing, balancing efficacy, safety, convenience, access, and preservation of future options. In this context, the most appropriate first-line therapy may not be defined by any single agent, but by how well it aligns with the patient’s clinical and personal priorities.
Presented by:
- Vignesh Packiam, MD, Director of Clinical and Translational Research in Urologic Oncology, Rutgers Cancer Institute of New Jersey, RWJ Barnabas Health, New Brunswick, NJ
- Amanda Myers, MD, MS, Assistant Professor, Department of Urology, University of Iowa, Iowa City, IA
- Bogdana Schmidt, MD, MPH, Assistant Professor, Department of Urology, University of Utah, Salt Lake City, UT
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Steinberg RL, Packiam VT, Thomas LJ, et al. Intravesical Sequential Gemcitabine and Docetaxel Versus Bacillus Calmette-Guérin Plus Interferon in Patients With Recurrent Non-Muscle Invasive Bladder Cancer Following a Single Induction Course of BCG. Urol Oncol. 2022;40(1):10.e1-10.e8.
- Chevuru P, McElree IM, Mott SL, et al. Long-Term Follow-Up of Sequential Intravesical Gemcitabine and Docetaxel Salvage Therapy for Non-Muscle Invasive Bladder Cancer. Urol Oncol. 2024;42(4):131.e17-131.e24.
- Pijpers OM, Bosch SG, van Diepen DC, et al. Intravesical Gemcitabine and Docetaxel in Patients With Recurrent High-Grade Nonmuscle Invasive Bladder Cancer: A Prospective Cohort Study. Eur Urol Oncol. 2025;8(4):603-611.
- Myers AA, Talwar R, Duan Z, et al. Cost-Effectiveness Analysis of Treatments for Bacillus Calmette-Guérin-Unresponsive Carcinoma In Situ of the Bladder. Eur Urol Oncol. 2025;8(2):314-322.