(UroToday.com) The American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, Nevada, was host to the Plenary Session on Saturday 26th of April. Drs. Tullika Garg, William Huang, Shreyas Joshi, Cheryl Lee, and Vignesh Packiam participated in a crossfire debate defending why double intravesical chemotherapy is preferred over newly FDA-approved agents for BCG-unresponsive non-muscle invasive bladder cancer (NMIBC).
Dr. Garg opened the session by referencing the current AUA guideline recommendations for patients with persistent or recurrent high-grade NMIBC within 12 months of completing adequate BCG therapy. For patients who are unwilling or unfit for cystectomy, clinicians may consider enrollment in clinical trials, alternative intravesical therapies such as nadofaragene (firadenovec-vncg), or doublet intravesical chemotherapies like gemcitabine/docetaxel. Systemic immunotherapy with pembrolizumab is also an option for patients with carcinoma in situ. However, it remains unclear what is the best agent to use.
This crossfire session was structured as a debate, with Drs. William Huang and Vignesh Packiam advocating for doublet intravesical chemotherapy, while Drs. Shreyas Joshi and Cheryl Lee presented arguments in favor of the newly FDA-approved agents.
Doublet Intravesical Chemotherapy: (Gemcitabine/Docetaxel)Dr. Packiam began his presentation by outlining the criteria for defining BCG-unresponsive NMIBC, emphasizing that patients must have received “adequate BCG,” commonly described by the “5+2” rule: at least 5 out of 6 induction doses and at least 2 out of 3 maintenance doses. BCG-unresponsive disease includes: (1) high-grade papillary (Ta/T1) recurrence within 6 months of the last BCG, (2) high-grade carcinoma in situ recurrence within 12 months, and (3) high-grade T1 recurrence at first evaluation (3 months) after a single BCG induction course. Patients not meeting these definitions are considered “BCG-exposed.”1
Carcinoma in situ (CIS) is highly recurrent and has become the priority NMIBC stage for FDA evaluation. CIS represents a field defect and is theoretically not surgically eradicable, making endpoints like anytime complete response (CR) and duration of response (DOR) important, yet impractical in clinical practice due to the challenges faced by both patients and urologists. Therefore, for assessing doublet intravesical chemotherapy with gemcitabine and docetaxel (Gem/Doce), and for consistency across studies, Dr. Packiam emphasized focusing on CIS patients and using 12-month landmark efficacy endpoints, such as CR, recurrence-free survival (RFS), and disease-free survival (DFS) should be our priority.
Gemcitabine is a nucleoside analog that inhibits DNA synthesis, while docetaxel is an anti-mitotic agent that inhibits tubulin disassembly. The treatment is administered sequentially, typically consisting of 1 g of gemcitabine infused over 60 minutes, followed by 37.5 mg of docetaxel over 60 minutes. The induction phase involves weekly instillations for six weeks, followed by a maintenance phase of monthly instillations for up to two years.
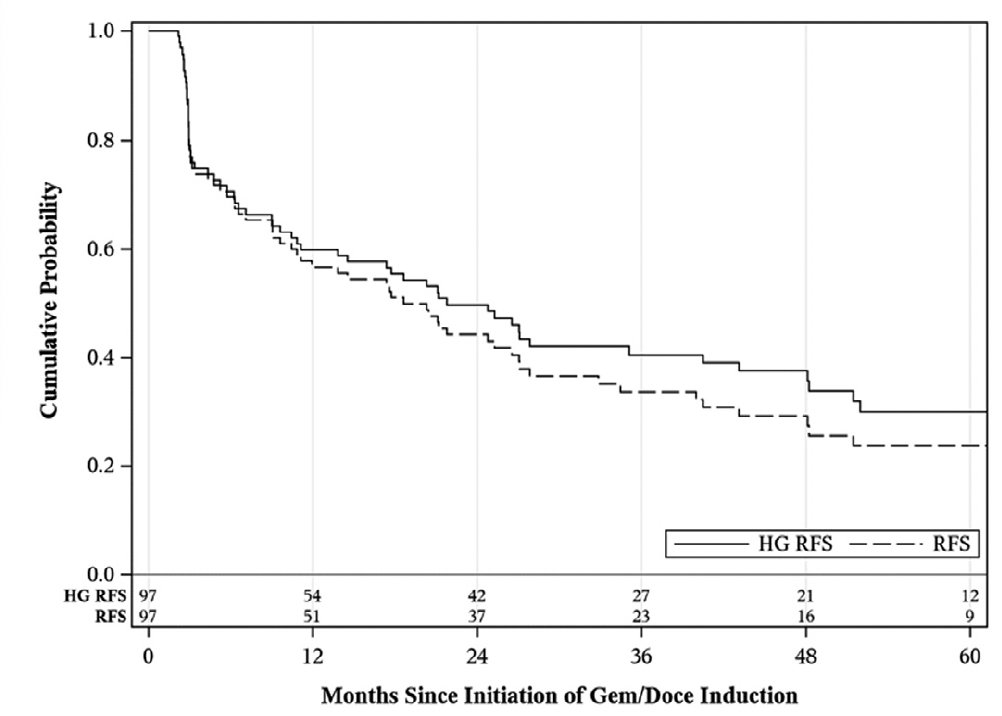
Dr. Packiam highlighted a landmark retrospective multicenter study conducted across seven institutions, which included 276 patients with BCG failure, of whom 38% met the definition of BCG-unresponsive disease and were treated with gemcitabine and docetaxel. Among the BCG-unresponsive CIS group, the one-year recurrence-free survival (RFS) was 60%, and the two-year RFS was 50%, as illustrated in the Kaplan-Meier curve below.2

Moreover, a single-institution study with long-term follow-up (median 49 months) evaluated 34 patients with BCG-unresponsive disease, including some with non-CIS histology. The authors reported a five-year recurrence-free survival of 28%, cystectomy-free survival (CFS) of 75%, and cancer-specific survival of 92%.3
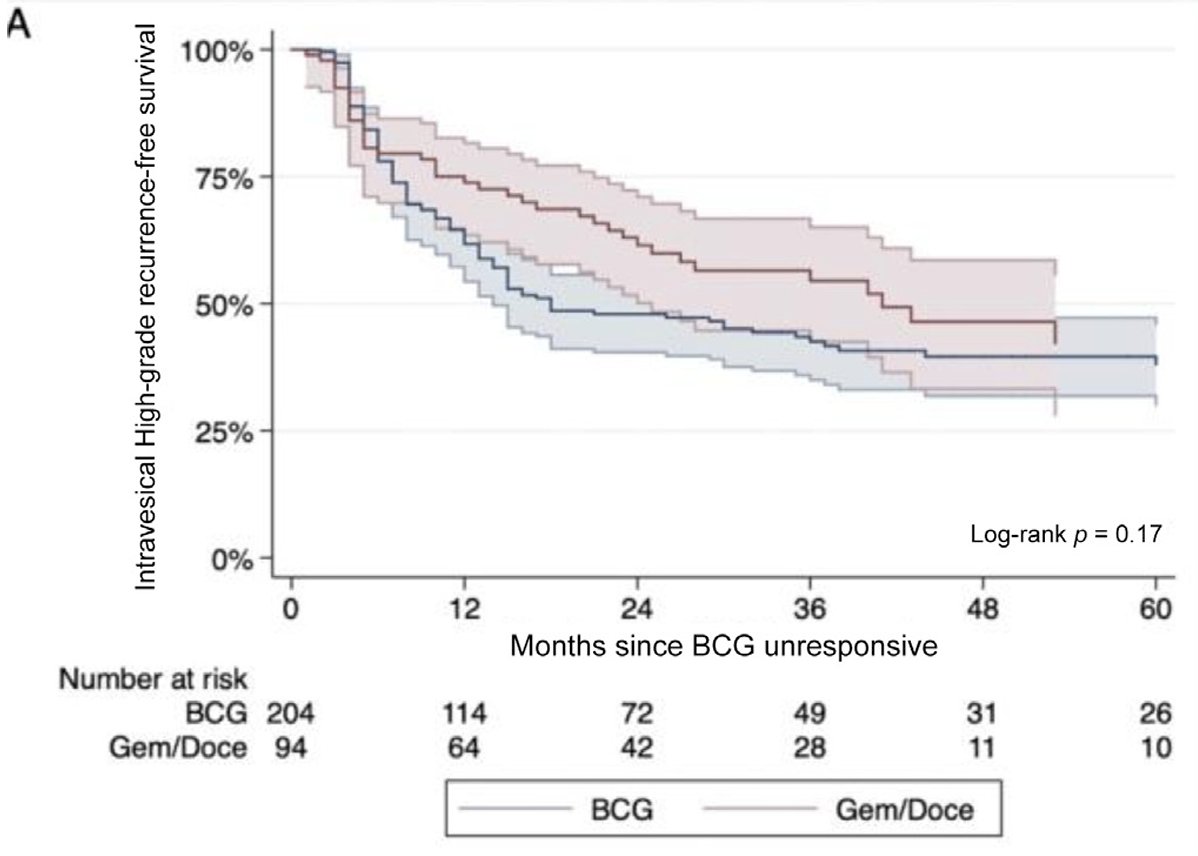
Dr. Packiam also highlighted a more contemporary study with long-term follow-up, conducted through a multinational, multi-institutional collaboration. This study assessed 299 patients with BCG-unresponsive disease, of whom 95 received gemcitabine/docetaxel. Among patients treated with gemcitabine/docetaxel, the high-grade recurrence-free survival (HG-RFS) rates were 63% at one year, 47% at two years, and 38% at five years.4
The question we should ask ourselves is whether gemcitabine/docetaxel is cost-effective. Dr. Packiam presented a cost-effectiveness analysis showing that gemcitabine/docetaxel remains cost-effective compared to radical cystectomy if the two-year recurrence-free survival is below 55%. Notably, pembrolizumab for BCG-unresponsive disease would never be considered cost-effective under current models. They also emphasized that newer therapies are likely to be even less cost-effective, given the rising associated costs.5

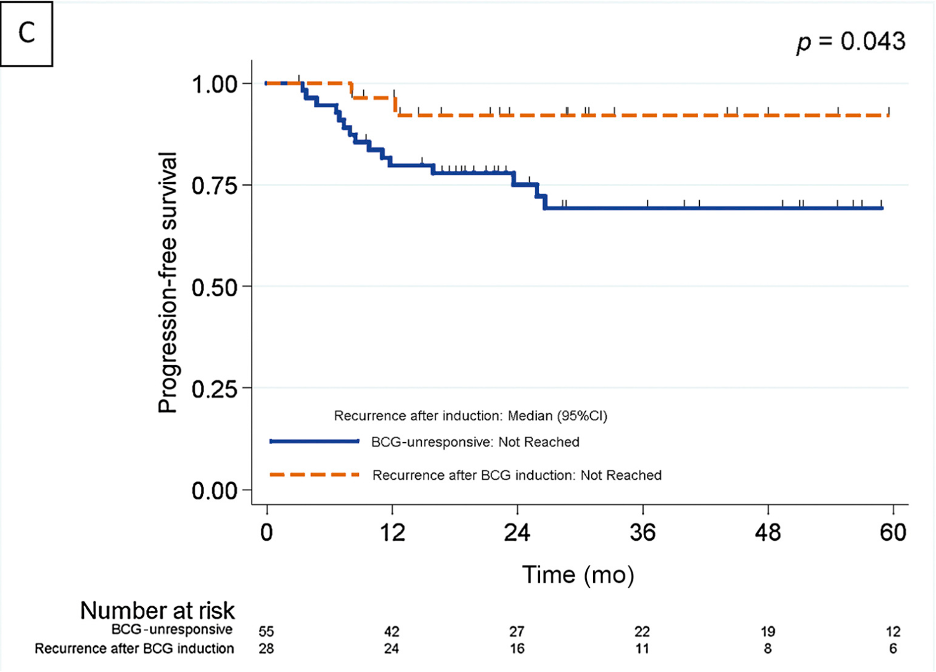
In a retrospective study of 312 patients with AUA high-risk NMIBC who were treatment-naïve, patients received either BCG (n=174; full dose or one-third dose with one year of maintenance) or gemcitabine/docetaxel (n=138). Notably, 40% of patients had carcinoma in situ, and more than 50% had T1 disease. The one-year CR rate for gemcitabine/docetaxel was an impressive 85%. Regarding tolerability, induction discontinuation rates were 2.9% for gemcitabine/docetaxel and 9.2% for BCG.6
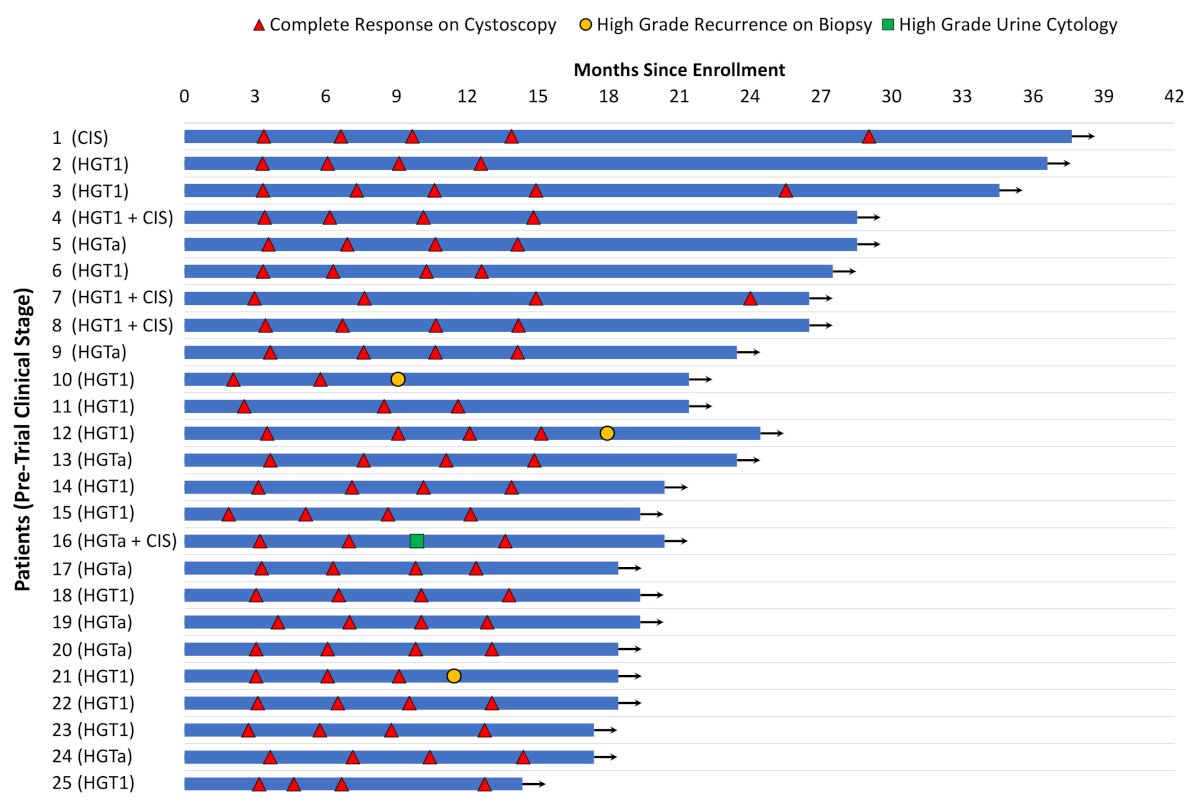
The largest criticism of Gem/Doce is that most data is retrospective however, similarly, in a prospective study of 25 treatment-naïve AUA high-risk NMIBC patients with a median follow-up of 19 months, the three-month CR rate was 100% and the one-year CR rate was 92%, as shown in the swimmer’s plot below.7
Dr. Joshi opened his portion of the debate by emphasizing that there is no "silver bullet" for BCG-unresponsive NMIBC. He noted that all of the panelists routinely use a combination of available agents to personalize care for their patients. While several therapies have received FDA approval, most are for patients with CIS, and it remains clear that we will not truly know the best treatment for each individual until biomarkers or more rational treatment algorithms are better developed.
The discussion then focused on three newer agents:
- Pembrolizumab (Keytruda)
- Nadofaragene firadenovec (Adstiladrin)
- Nogapendekin alfa inbakicept-pmln (Anktiva)
We should be treating and counseling patients based on the highest level of evidence, prospective clinical trials with comprehensive reporting of outcomes, side effects, and landmark CR data at defined timepoints. Given the explosion of potential new therapies, now is the time to follow the best available evidence for NMIBC. Encouragingly, we now have three prospective, multi-institutional, multinational, well-designed studies available in this disease space.
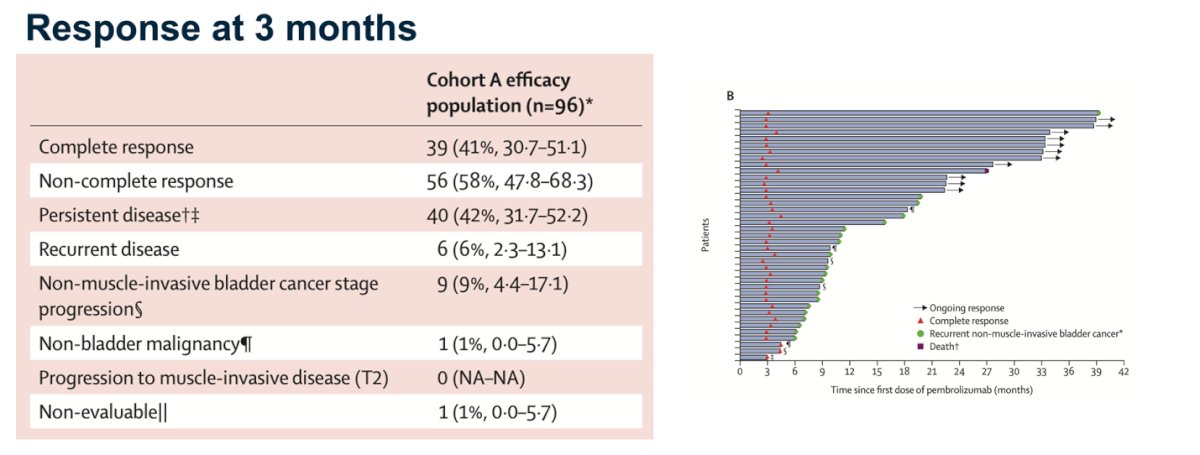
Pembrolizumab is a PD-1 inhibitor administered via systemic infusion. Data supporting its use come from an open-label, single-arm, multicenter phase 2 study. Notably, while there are multiple lines of therapy in this disease space, pembrolizumab was the first FDA-approved agent but is not considered a first-line treatment. Presenting the agents in the order of FDA approval, the KEYNOTE-057 study showed a CR rate of 39% at 3 months in Cohort A, which included patients with CIS.8
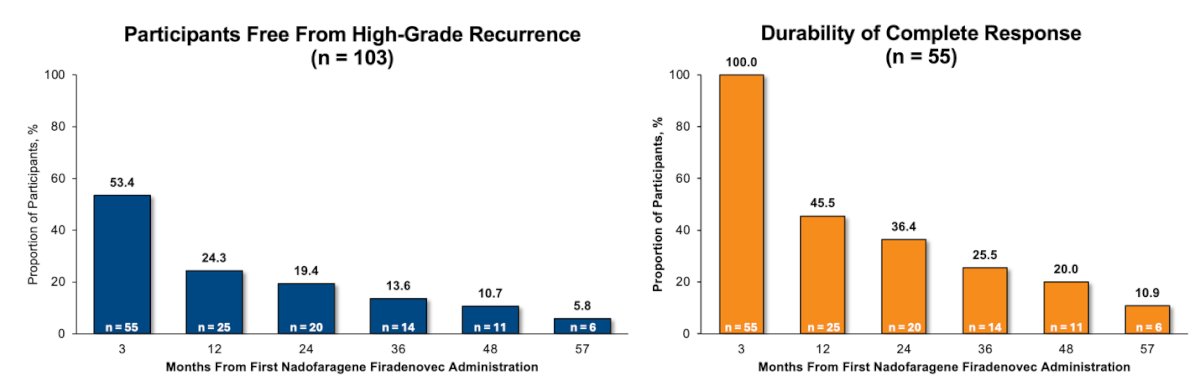
Nadofaragene firadenovec is an adenoviral gene therapy targeting the interferon pathway, administered via intravesical instillation. It was evaluated in a single-arm, open-label, repeat-dose clinical trial in participants with CIS, with or without associated Ta or T1 disease. Notably, 5.8% of participants (6/103) with CIS ± Ta/T1 were high-grade recurrence-free (HGRF) at 57 months. Among those who achieved a CR CR at 3 months, 10.9% (6/55) remained HGRF at 57 months, as shown below.9
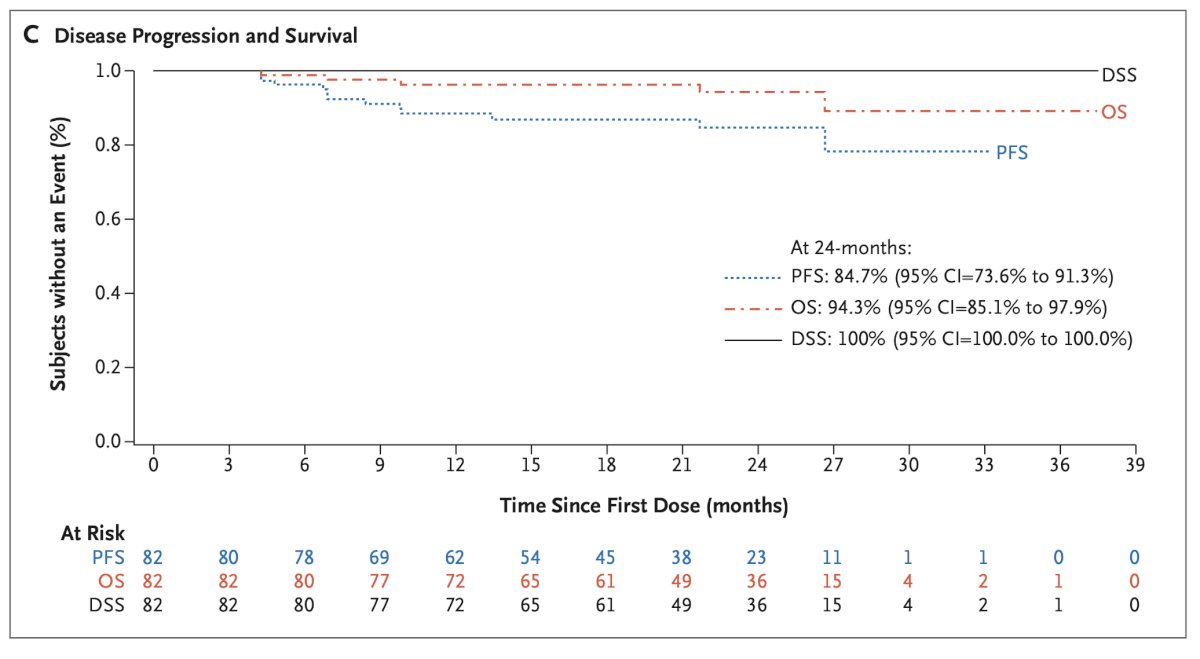
Nogapendekin alfa inbakicept-pmln (Anktiva) is an IL-15 super-agonist administered intravesically in combination with BCG. Notably, it demonstrated a 71% CR at any time during follow-up, with CR rates of 55% at 3 months, 56% at 6 months, 45% at 12 months, and 33% at 18 months. The therapy also showed durable disease-specific survival (DSS), overall survival (OS), and progression-free survival (PFS). At 24 months, the PFS was 84.7%, OS was 94.3%, and DSS remained at 100%.10
It is important to understand the logistics of administration for each of these new treatments. Pembrolizumab is given every three weeks as a 30-minute infusion, which is particularly favorable for patients with poor bladder tolerance. Adstiladrin is administered every three months through a one-hour intravesical instillation and is generally very well tolerated. Anktiva is co-administered with BCG, which simplifies logistics given that urology clinics already have extensive experience with BCG administration. In contrast, gemcitabine/docetaxel regimens require a greater logistical burden, occupying a clinic room and nursing staff for approximately two hours weekly over six weeks for each patient, followed by monthly maintenance for up to two years. Ultimately, there is a necessary trade-off between optimizing patient satisfaction and maintaining workflow efficiency for urology practices.
More importantly, we now have long-term survival data, with five-year follow-up available from the pivotal trials. This is critical, as it helps inform patient care decisions and set real expectations. For pembrolizumab, five-year follow-up data from KEYNOTE-057 were presented. Among the 96 patients treated, the median follow-up was 58.0 months (range: 4.6–72.5 months). Notably, 23.1% (9/39) of responding patients maintained a CR for 45 months or longer, with the duration of response for these patients ranging from 46.9 to 57.7 months.
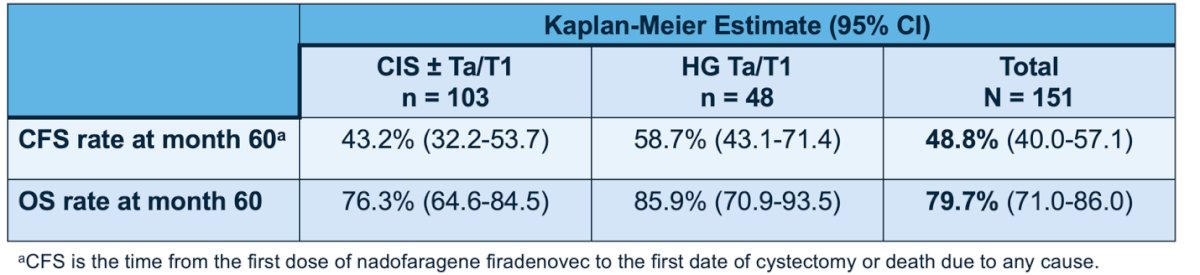
Similarly, for Adstiladrin (nadofaragene firadenovec), we have very important prospective data that we can use when counseling our patients. Notably, in this study, the five-year data are encouraging. The cystectomy-free survival rate at 60 months in the overall cohort was 48.8%, and the OS rate at 60 months was 79.7%.
Dr. Joshi emphasized that we should capitalize on the immunologically sensitive biology of bladder cancer. All three alternatives rely on activating the immune system as a therapeutic strategy, reinforcing the most well-established treatment pathway for high-risk NMIBC. Importantly, each agent has the potential to induce immunologic memory and sustain an adaptive immune response even after treatment is completed, something traditional chemotherapies are unable to achieve.
Dr. Joshi concluded his presentation by encouraging the audience to consider these new agents thoughtfully. He stressed the importance of following the evidence and basing treatment decisions on the highest-level data available. He also highlighted the need to weigh logistical advantages, such as treatment intervals, urologist comfort with administration, and options for patients who may not tolerate prolonged intravesical instillations. Lastly, he underscored that with emerging long-term data, we are now better equipped to inform patients about their likelihood of success out to five years and to fully leverage the immuno-sensitivity of bladder cancer to build durable, adaptive immune responses.
Doublet Intravesical Chemotherapy: (Gemcitabine/Docetaxel): RebuttalDr. Huang began his portion of the debate by highlighting that, for decades, the “price of success” in this disease space and for these patients is undergoing radical cystectomy, but there are certainly many unmet needs in this field. There is no prospective long-term data for gemcitabine-docetaxel, there is a reasonable amount of long-term real-world and retrospective data supporting its use. He noted that one way to compare the "price of success" between doublet intravesical chemotherapy and the newer agents is by assessing radical cystectomy-free survival.
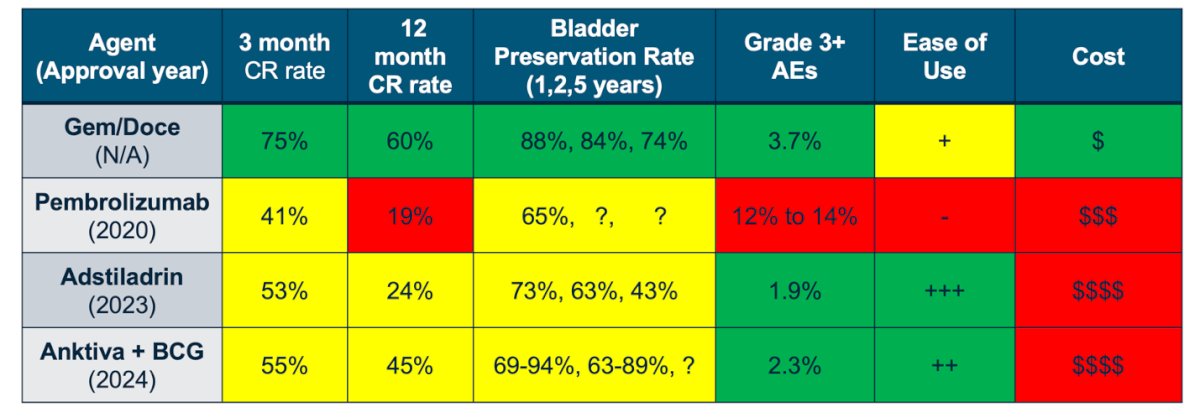
In terms of efficacy, the table below summarizes the 3-month CR rate, 12-month CR rate, and bladder preservation rates. Notably, the 3-month and 12-month CR rates are highest in the doublet intravesical chemotherapy group. Additionally, bladder preservation rates with this approach remain superior at one, two, and five years.

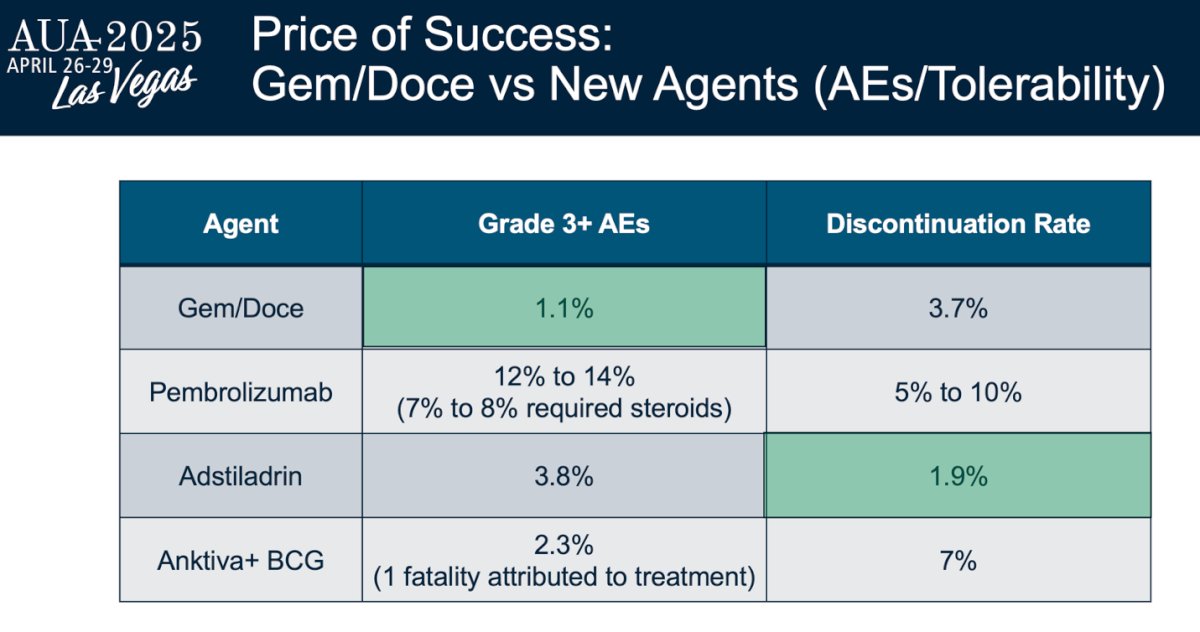
In terms of adverse events and tolerability, gemcitabine-docetaxel demonstrated the lowest rate of grade 3 adverse events among all treatments. Its discontinuation rate was also favorable, ranking second lowest after Adstiladrin, which reported a discontinuation rate of just 1.9%.
Gemcitabine-docetaxel provides several practical advantages, including ease of use and provider familiarity with intravesical instillation protocols. It does not require concurrent BCG administration, offers prolonged dwell times for enhanced exposure, and fits into well-established chemotherapy workflows in urology clinics.
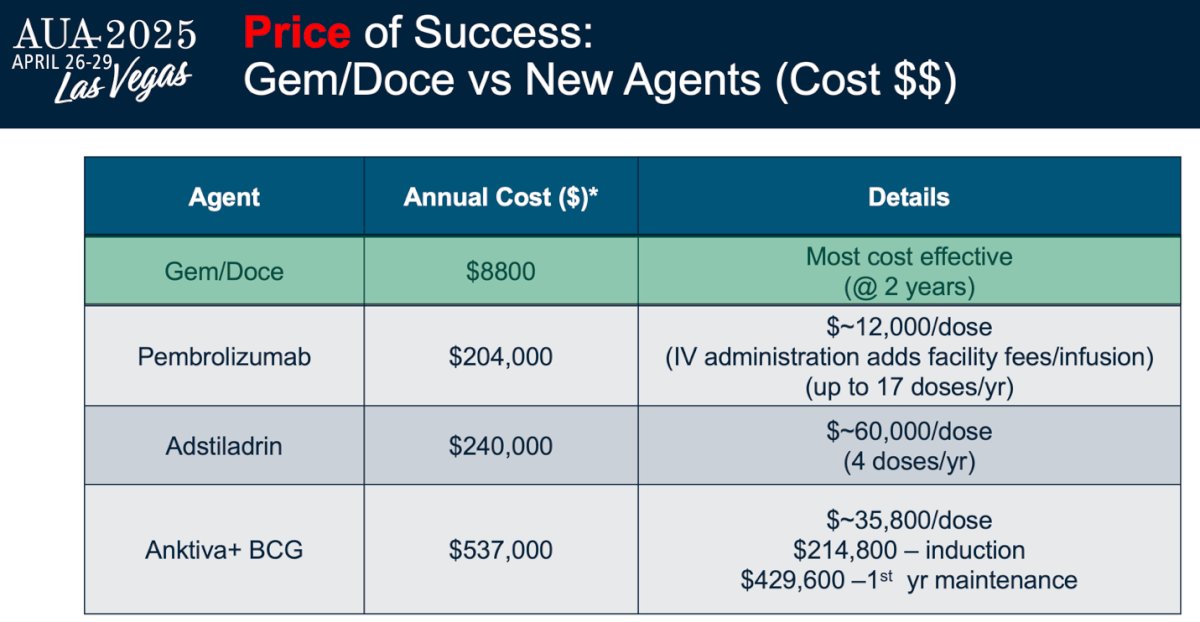
Moreover, the annual cost associated with gemcitabine-docetaxel was significantly lower at $8,800 (20 times less), making it the most cost-effective treatment at two years, as shown in the table below.
Dr. Huang concluded his presentation by summarizing the data in the table below, highlighting that gemcitabine-docetaxel outperforms the newly FDA-approved treatment options in 3- and 12-month complete response rates, bladder preservation rates, overall cost, and also maintains a low rate of grade 3 adverse events and highlighted that in 2025, should be the preferred treatment of choice.
Dr. Lee pointed out that the full breadth of prospective data for gemcitabine-docetaxel in BCG-unresponsive patients is, in fact, nonexistent. While there is a growing body of data in the BCG-naïve setting, it remains limited to just 25 patients. She emphasized the importance of carefully examining the data and urged caution due to the inherent biases of retrospective studies especially in the bladder cancer space. As an example, she cited the SWOG S1011 trial, where extended lymph node dissection did not improve survival compared to standard lymph node dissection, findings that contrast with earlier retrospective reports.
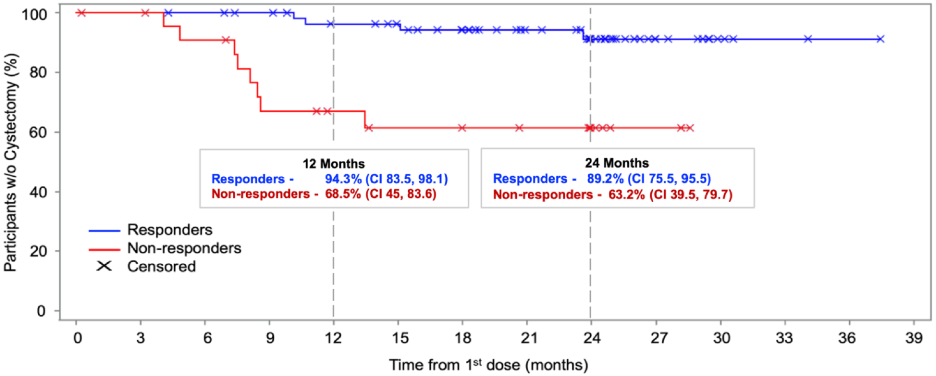
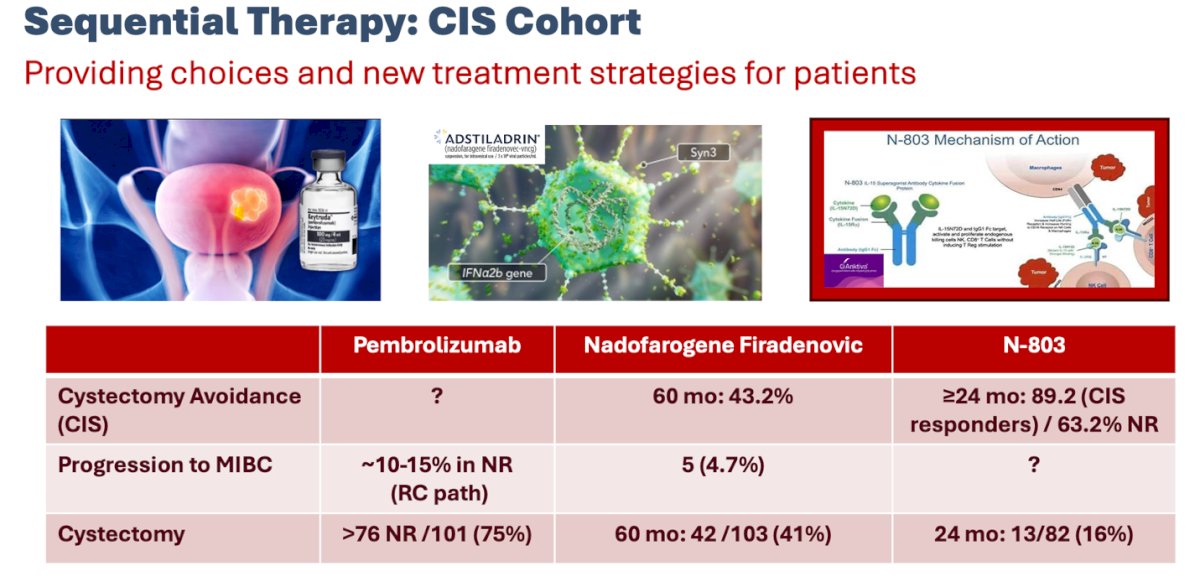
Dr. Lee highlighted that while there is a cost associated with these new agents, there is also an inherent cost to innovation. However, when considering data such as that from the N-803 (nogapendekin alfa inbakicept) study combined with BCG, the outcomes are highly encouraging. This study demonstrated a 24-month cystectomy avoidance rate of 89% among responders, with disease-specific survival (DSS) at 100% and overall survival (OS) at 94.3%.10
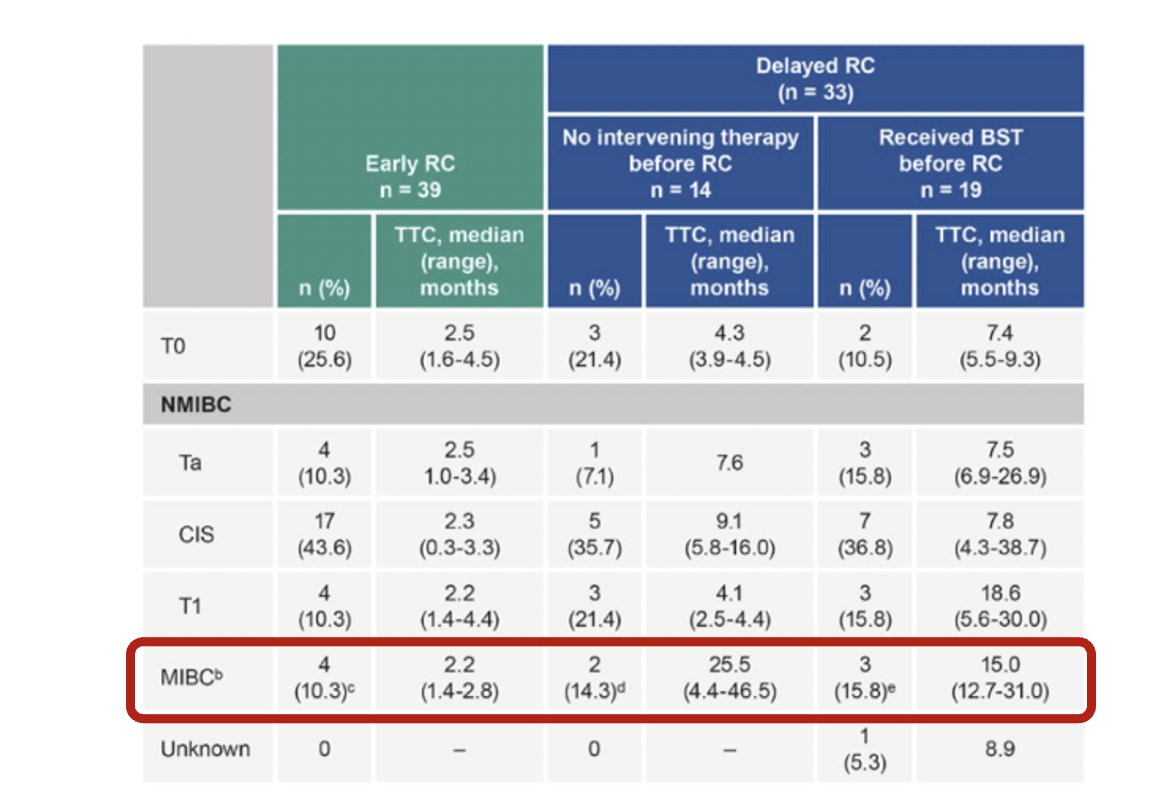
One important point Dr. Lee addressed was the role of cystectomy after pembrolizumab. She presented a post hoc analysis evaluating whether third-line therapy is feasible in carefully selected patients. The analysis found that participants who underwent early versus delayed radical cystectomy had similar pathological outcomes, suggesting that salvage cystectomy remains a viable option for non-responders.11
Moreover, these agents may offer a more convenient dosing schedule. For example, Nadofaragene offers a more convenient dosing schedule, it is administered intravesically every three months for a total of five doses. In contrast, gemcitabine-docetaxel requires 15 intravesical instillations, each lasting 2–4 hours. As has been consistently shown, treatment intensity can be particularly burdensome for both patients and their families.

Lastly, we should acknowledge the costs of these novel FDA-approved therapies, however, it is essential to offer our patients meaningful choices and explore new treatment strategies for sequential therapy after BCG failure. These approaches should aim to avoid cystectomy and prevent progression to muscle-invasive disease, as highlighted below.
Dr. Garg concluded their crossfire debate by emphasizing several key points:
- All treatment options come with associated costs, financial, adverse events, treatment burden, and impact on clinical operations.
- We are entering a paradigm-shifting, game-changing era for BCG-unresponsive NMIBC, with new therapies focused on preserving both the bladder and patients' quality of life.
- This is not a competition between therapies, but rather an opportunity to build a full armamentarium of agents with multiple mechanisms of action.
- Moving forward, there is a critical need to develop treatment algorithms to guide the sequencing of these new agents.
Presented by:
- Tullika Garg, MD, MPH, FACS, Urologic Oncologist at Penn State Health Milton S. Hershey Medical Center, Dept. of Urology, Hershey, PA
- William Huang, MD, Urologic oncologist at NYU Langone Health and the Perlmutter Cancer Institute. New York, NY.
- Shreyas Joshi, MD, MPH, Assistant Professor in the Department of Urology at the Emory University School of Medicine. Atlanta, GA.
- Cheryl Lee, MD, Urologic Oncologist at the Ohio State University Comprehensive Cancer Center (OSUCCC), Columbus, OH.
- Vignesh Packiam, MD, Associate Professor of Urologic Oncology and Director of Clinical and Translation Research in Urologic Oncology at Rutgers Cancer Institute of New Jersey. New Brunswick, NJ.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, NV.
References:
- Kamat AM, Sylvester RJ, Böhle A, Palou J, Lamm DL, Brausi M, Soloway M, Persad R, Buckley R, Colombel M, Witjes JA. Definitions, End Points, and Clinical Trial Designs for Non-Muscle-Invasive Bladder Cancer: Recommendations From the International Bladder Cancer Group. J Clin Oncol. 2016 Jun 1;34(16):1935-44. doi: 10.1200/JCO.2015.64.4070. Epub 2016 Jan 25. PMID: 26811532; PMCID: PMC5321095.
- Steinberg RL, Thomas LJ, Brooks N, Mott SL, Vitale A, Crump T, Rao MY, Daniels MJ, Wang J, Nagaraju S, DeWolf WC, Lamm DL, Kates M, Hyndman ME, Kamat AM, Bivalacqua TJ, Nepple KG, O'Donnell MA. Multi-Institution Evaluation of Sequential Gemcitabine and Docetaxel as Rescue Therapy for Nonmuscle Invasive Bladder Cancer. J Urol. 2020 May;203(5):902-909. doi: 10.1097/JU.0000000000000688. Epub 2019 Dec 10. PMID: 31821066.
- Chevuru PT, McElree IM, Mott SL, Steinberg RL, O'Donnell MA, Packiam VT. Long-term follow-up of sequential intravesical gemcitabine and docetaxel salvage therapy for non-muscle invasive bladder cancer. Urol Oncol. 2023 Mar;41(3):148.e1-148.e7. doi: 10.1016/j.urolonc.2022.10.030. Epub 2022 Nov 28. PMID: 36456454.
- Taylor J, Kamat AM, Annapureddy D, Khene ZE, Howard J, Tan WS, McElree IM, Facundo D, Yim K, Harrington S, Dyer E, Black AJ, Kanabur P, Roumiguié M, Lerner S, Black PC, Raman JD, Preston M, Steinberg G, Huang W, Li R, Packiam VT, Woldu SL, Lotan Y, O'Donnell MA. Oncologic Outcomes of Sequential Intravesical Gemcitabine and Docetaxel Compared with Bacillus Calmette-Guérin in Patients with Bacillus Calmette-Guérin-Unresponsive Non-Muscle Invasive Bladder Cancer. Eur Urol Oncol. 2025 Apr;8(2):469-476. doi: 10.1016/j.euo.2024.12.005. Epub 2024 Dec 17. PMID: 39694798.
- Wymer KM, Narang G, Slade A, Sharma V, Thao V, Borah BJ, Rivera M, Cheney S, Humphreys MR. Evaluation of the Cost-Effectiveness of Surgical Treatment Options for Benign Prostatic Hyperplasia. Urology. 2023 Jan;171:96-102. doi: 10.1016/j.urology.2022.09.026. Epub 2022 Oct 19. PMID: 36270339.
- McElree IM, Steinberg RL, Mott SL, O'Donnell MA, Packiam VT. Comparison of Sequential Intravesical Gemcitabine and Docetaxel vs Bacillus Calmette-Guérin for the Treatment of Patients With High-Risk Non-Muscle-Invasive Bladder Cancer. JAMA Netw Open. 2023 Feb 1;6(2):e230849. doi: 10.1001/jamanetworkopen.2023.0849. PMID: 36853609; PMCID: PMC9975907.
- Patel SH, Gabrielson AT, Chan S, Schwartz D, Collins C, Singla N, Trock B, Bivalacqua TJ, Hahn N, Kates MR. A Phase 2 Trial of Intravesical Gemcitabine and Docetaxel in the Treatment of Bacillus Calmette-Guérin‒Naïve Nonmuscle-Invasive Urothelial Carcinoma of the Bladder. J Urol. 2024 Jul;212(1):95-103. doi: 10.1097/JU.0000000000003977. Epub 2024 Apr 23. PMID: 38653234.
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non–muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): a multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. 2021;22(7):919-930. doi:10.1016/S1470-2045(21)00235-8
- Boorjian SA, Alemozaffar M, Konety BR, et al. Nadofaragene firadenovec for BCG-unresponsive non–muscle-invasive bladder cancer: a phase 3, multicentre, open-label, repeat-dose study. Lancet Oncol. 2021;22(7):107–117. doi:10.1016/S1470-2045(20)30740-0
- Chamie K, Palmer-Aronsten B, Masson-Lecomte A, et al. Nogapendekin alfa inbakicept with BCG for patients with BCG-unresponsive non–muscle-invasive bladder cancer: primary results from the phase 2/3 QUILT 3.032 trial.Nat Med. 2024;30(3):623–632. doi:10.1038/s41591-024-02862-9
- Li R, Kamat AM, Kwon D, et al. Outcomes of patients with BCG-unresponsive high-risk non–muscle-invasive bladder cancer who demonstrated nonresponse to pembrolizumab in KEYNOTE-057: A post hoc analysis. J Clin Oncol.2024;42(16_suppl):4597. doi:10.1200/JCO.2024.42.16_suppl.4597.