(UroToday.com)The 2023 AUA annual meeting included the Bladder Cancer Forum, featuring a debate discussing whether skilled urologists need PDD to perform an optimal TURBT. Dr. Neal Shore started his talk by presenting a case of a 63 year old African Caribbean female with asymptomatic microhematuria (10-12 rbc/hpf).
Her medical history was notable for poorly managed hypertension and she had a 20 pack year smoking history and 40 year history of rum production (sugar cane and molasses). Regarding her family history, her father died of prostate cancer at 60 years of age and her mother died of breast cancer at 55 years of age. Her CT urogram was unremarkable, urine biomarkers were not sent, and cystoscopy was scheduled. Dr. Shore then polled the audience for “What percentage of urologists who perform TURBT do you consider skilled”?
- 100% (4% of respondents)
- >50% (51% of respondents)
- <50% (28% of respondents)
- Unsure what “skilled” means (18% of respondents)
Additionally, 53% of the audience noted that they had access to PDD, 36% responded that they have access to PDD and use it routinely, and 36% said they did not have access to PDD but would like access (38% did not want access and 26% said they were unsure).
Dr. Michael Cookson then presented, taking the position that no, skilled urologists do not really need blue light cystoscopy. Dr. Cookson emphasizing what he is not trying to refute with regards to non-muscle invasive bladder cancer:
- In most large RCTs, blue light cystoscopy enhances detection of papillary and flat lesions
- In most large RCTs, blue light cystoscopy reduces recurrence rates
- Blue light cystoscopy is endorsed by major guidelines
- In large RCTs and in real world experience, blue light cystoscopy does not reduce progression to muscle invasion
It is important to emphasize that blue light cystoscopy should be used in conjunction with white light cystoscopy, not as a replacement. In a multicenter study, 311 patients with known or suspected bladder cancer, blue light cystoscopy missed 9% of tumors visualized by white light cystoscopy, including 5% of T1 tumors.1 In the same study, blue light cystoscopy detected at least one additional tumor compared with white light cystoscopy in 29% of patients and detected at least one additional T1 tumor in 15% of patients. Thus, both white light and blue light must be used in the same patient to obtain maximum benefit.
Dr. Cookson notes that he is here to inform us with regards to:
- In a recent large, practical multicenter RCT, blue light cystoscopy did not reduce the rate or recurrence and was not cost-effective
- In the US, despite more than a decade of approval and opportunity, blue light cystoscopy has not been adopted by most experienced urologists and has been abandoned by some early adopters
- Barriers to adoption, unfavorable economics, and potential loss of access to flexible equipment will continue to relegate use to academic and select large volume centers
The PHOTOdynamic trial was a pragmatic, open-label, parallel-group randomized trial conducted in 22 UK hospitals (n=538), with a suspected first diagnosis of NMIBC at intermediate or high risk for recurrence based on routine visual assessment before being listed for TURBT.2 Participants were assigned (1:1) to PDD-guided TURBT or to standard white light–guided TURBT. The primary clinical outcome was time to recurrence at 3 years of follow-up, analyzed by modified intention to treat. After a 44 month median follow-up, 86 of 209 in the PDD group and 84 of 217 in the white-light group had recurrences. The hazard ratio for recurrence was 0.94 (95% CI, 0.69 to 1.28; p=0.70):
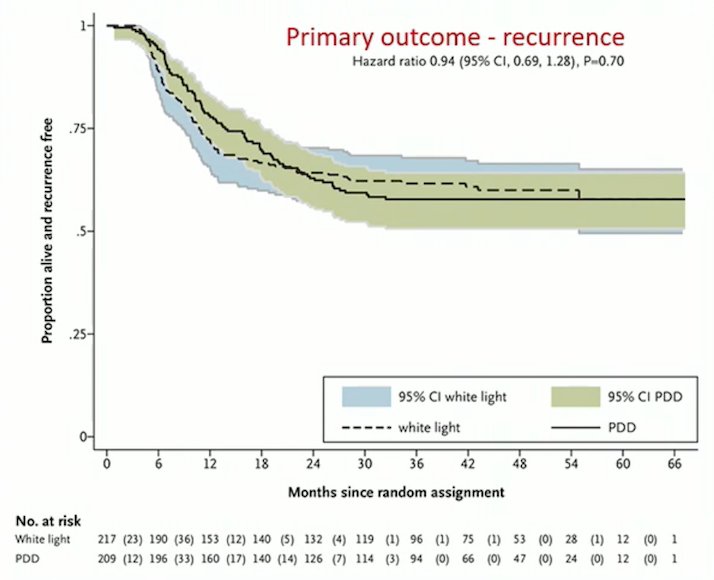
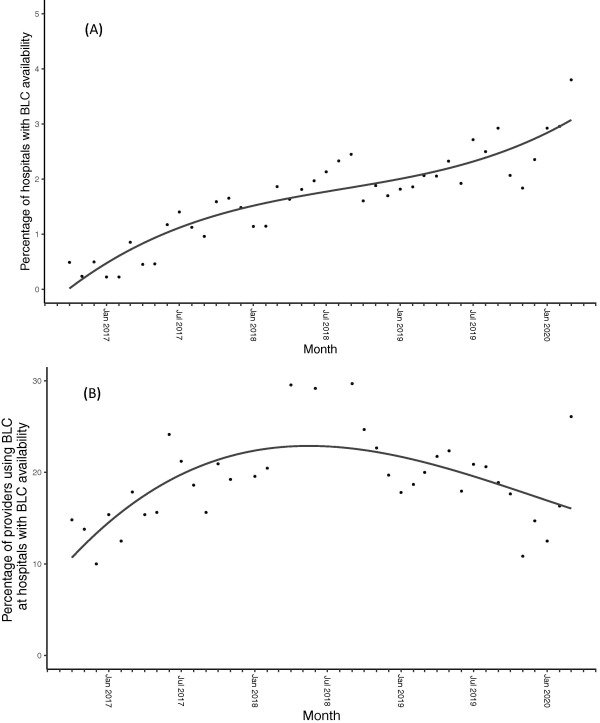
This trial concluded that PDD-guided TURBT did not reduce recurrence rates, nor was it cost-effective compared with white-light TURBT at 3 years. Data from the Premier Healthcare Database, a large national sample of data, suggests underutilization of blue light cystoscopy for bladder cancer in the US.3 Among 158,870 patients undergoing TURBT between January 2011 and March 2020, blue light cystoscopy was used in 1.2% of TURBTs over the study period, with use increasing following the AUA NMIBC guidelines being published in October 2016, but plateauing in late 2018.

After adjusting for patient characteristics, higher odds for blue light cystoscopy use were found at academic hospitals and hospitals with higher TURBT volumes and higher radical cystectomy volumes. As follows is the percentage of hospitals with blue light cystoscopy availability (A) and percentage of providers using blue light cystoscopy at hospitals with blue light cystoscopy availability over time (B):
Reasons for decreasing blue light cystoscopy are likely multifactorial, including complex equipment and expense. Dr. Cookson notes that the net increase in total costs of care has been calculated at $110.09 per cystoscopy for blue light cystoscopy. However, cost-effectiveness studies for blue light cystoscopy have several model limitations:
- Assumes non-muscle invasive disease management would follow published guidelines, whereas in the real-world setting, there would be variation based on both patients and physicians
- Risk of recurrence in the first year and second year would be identical
- Does not calculate clinical outcomes and economic impact of false positives
- Assumed the complete transition of patients from white light cystoscopy assessment to blue light cystoscopy, which is unlikely in real world clinical practice given patient or urologist preferences
- Assumed an ASC site, whereas in the real-world there is a mix of different sites (office-based, ASC, or hospital outpatient) based on patient characteristics or availability of care settings
- Added costs due to progression with the white light cystoscopy cohort, if recurrences remain undetected, assumes all missed recurrence progresses, which represents the upper limit of financial risk for added costs
Furthermore, the flexible endoscopy indication recently took a massive step back in 2023 with Storz announcing discontinuation of the flexible blue light cystoscopy tower production in the United States. A complete time line of the blue milestones is as follows:

Dr. Cookson concluded his portion of the debate emphasizing that no, skilled urologists do not need PDD, with the following concluding statements:
- Reduction in recurrence is not as significant in expert hands
- Investment in flexible blue light cystoscopy is now a sunk cost
- There is no impact on progression or overall survival
- There is recognition of underutilization in the United States
- Cost of equipment is substantial and potentially unrecoverable
- There may be a role for judicious and selective use of blue light cystoscopy technology
Dr. Trinity Bivalacqua then presented, taking the position that yes, skilled urologists do need blue light cystoscopy. Dr. Bivalacqua notes that what he is not here to refute in NMIBC is the cost-effectiveness of flexible blue light cystoscopy or the impact on progression to MIBC and overall survival. However, what he is here to inform on is:
- Defining optimal TURBT and skilled surgeons
- Critical review of the PHOTO trial
- Cost effectiveness of blue light cystoscopy over time
- The effect on health related quality of life in bladder cancer patients undergoing blue light cystoscopy
The definition of an optimal TURBT is an 8 mm margin of tumor free urothelium around the lesion, which decreases local recurrence rate from 58% to 19%. Additionally, multiple studies have shown that experienced surgeons perform a more complete resection and have lower recurrence rates, compared to those with less experience.
Regarding his critical review of the PHOTO trial, Dr. Bivalacqua emphasized that this truly was a pragmatic trial; moreover, results were only presented for 426 of 538 patients enrolled in the trial. Second, the primary endpoint was evaluated at 36 months, whereas previous RCTs have shown benefit for low and high grade recurrence at 12 months. Third, the PHOTO trial suggest that blue light (PDD) has little benefit in newly diagnosed intermediate NMIBC. However, we are unable to make blanket conclusions about the value to blue light-guided TURBT for recurrent or high-risk disease. Fourth, the study was underpowered and adjuvant therapy was not uniform between groups; 63.6% of blue light cystoscopy received adjuvant therapy, 79.7% of the white light cystoscopy patients (BCG use: 31.8% for blue light cystoscopy versus 46.0% for white light cystoscopy). The trial was underpowered, as it was powered to show a relative risk reduction of 30% 3 year recurrence rate, and 214 events were necessary, however only 170 events were detected. There were 107 patients (20%) that were excluded because of diagnostic misclassification based on white light cystoscopy. Exclusion of patients after randomization because of retrospective review increases the risk of selection bias and statistical results, thus this is more of a per protocol analysis.
For health related quality of life, a phase 3, multi-center study in which PROMS questionnaires were administered at baseline after surveillance with blue light cystoscopy and after TURBT found that there were decreased anxiety levels after blue light cystoscopy, with a greater decrease among those with negative pathology results (p = 0.051).4
Dr. Bivalacqua concluded his portion of the debate emphasizing that yes, skilled urologists need PDD, with the following concluding statements:
- Blue light cystoscopy improves health related quality of life in NMIBC patients
- There is a large body of evidence to support blue light cystoscopy with major concerns about the PHOTO trial design and patient population
- We must acknowledge the potential underutilization in the US
- The cost of equipment is substantial, but recovered over time; there may be potential unrecoverable costs in low volume center
- We must employ judicious and selective use of blue light cystoscopy technology, with target populations likely those with high risk NMIBC
Moderator: Neal D. Shore, MD, FACS, Medical Director, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC
Debater: Trinity J. Bivalacqua, MD, PhD University of Pennsylvania, Perelman Center, Philadelphia, PA
Debater: Michael S. Cookson, MD, University of Oklahoma, Oklahoma City, OK
Written By: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2023 American Urological Association (AUA) Annual Meeting, Chicago, IL, April 27 – May 1, 2023
References:
- Grossman HB, Gomella L, Fradet Y, et al. A phase III, multicenter comparison of hexaminolevulinate fluorescence cystoscopy and white light cystoscopy for the detection of superficial papillary lesions in patients with bladder cancer. J Urol. 2007;178(1): 62-67.
- Heer R, Lewis R, Vadiveloo T, et al. A randomized trial of PHOTOdynamic Surgery in Non-Muscle-Invasive Bladder Cancer. NEJM Evid 2022;1(10).
- Lewicki P, Arenas-Gallo C, Qiu Y, et al. Underutilization of blue light cystoscopy for bladder cancer in the United States. Eur Urol Focus. 2022;8(4):968-971.
- Smith AB, Daneshmad S, Patel S, et al. Patient-reported outcomes of blue-light flexible cystoscopy with hexaminolevulinate in the surveillance of bladder cancer: Results from a prospective multicentre study. BJU Int 2019;123:35-41
Related Content:
Optimal TURBT: Do Skilled Urologists Really Need Photodynamic Diagnosis (PDD)? -Trinity Bivalacqua & Michael Cookson