For this study, men diagnosed with clinically significant localized prostate cancer who were suitable for either robotic-assisted radical prostatectomy or radiotherapy were eligible for recruitment. Participants attended a combined clinic at a tertiary referral centre (Liverpool Hospital, Sydney), where they consulted a urologist and radiation oncologist regarding treatment options. Initial treatment preferences and final treatment choices were collected via questionnaires and consultations at the combined clinic were audio-recorded and transcribed verbatim. A subset of participants completed semi-structured interviews outlining their beliefs, values and decision-making process. Interviews were thematically analyzed and a mixed-methods design was used.
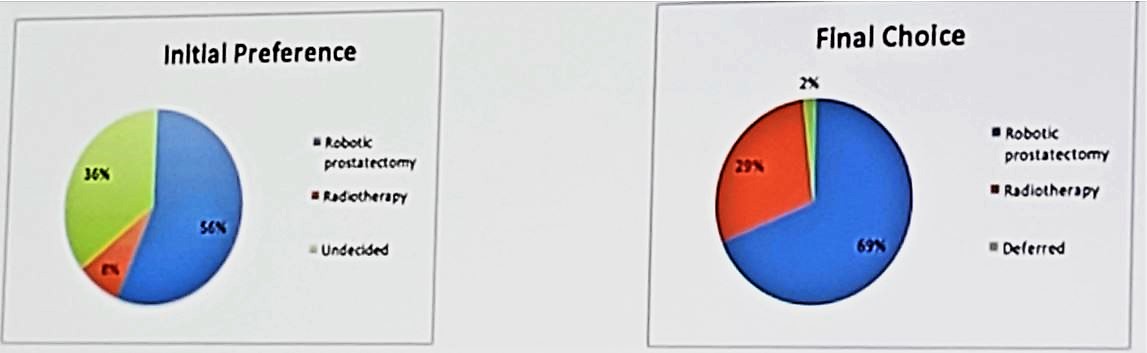
There were 41 patients who were consented to participate in this study (n=2 declined; n=3 non-responders). The mean age was 66 years old and mean pre-op PSA was 9.1 ng/mL. The most prevalent grade was ISUP grade II (47%) followed by ISUP III (19%). Twenty-eight (68%) participants ultimately chose robotic prostatectomy, 12 (29%) chose radiotherapy, and 1 (2%) deferred treatment. Initial treatment preference was recorded in 36 patients. There were 17 out of 21 (81%) patients with an initial preference ultimately retained their original choice, while 4 (19%) patients changing their preference from radical prostatectomy to radiation therapy. In the 13 patients who were unsure about treatment before the combined clinic, eight subsequently chose robotic prostatectomy and five chose radiation therapy.
Interviews revealed that treatment choice is largely dependent on clinicians’ recommendations and participants did not routinely compare specific side effects of each treatment. In patients who were undecided or changed preference, factors which played a significant role in decision-making included treatment delivery, side effects, age and comorbidities (71% of patients). There was a strong patient belief that robotic prostatectomy provided a more definitive cure (74% of robotic prostatectomy patients), while older men preferred radiotherapy as it had a perceived lesser impact on lifestyle (66% of radiotherapy patients). A limitation of this study is that all participants had to attend the combined clinic to be eligible for robotic prostatectomy via the public health system, which may result in selection bias of patients desiring surgical intervention. Second, men who elected for watchful waiting/active surveillance or decided to pay for a robotic prostatectomy in the private system are not represented.
Dr. Nalavenkata concluded his presentation with several remarks:
- Men who already had an initial treatment preference were unlikely to change their ultimate decision following the combined clinic consultation.
- In undecided patients, tailored discussion focusing on patient and treatment factors contributed to their treatment choice.
- Early involvement in a combined clinic can benefit the undecided patient in making a balanced and informed decision.
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University - Medical College of Georgia, @zklaassen_md at American Urological Association's 2019 Annual Meeting (AUA 2019), May 3 – 6, 2019 in Chicago, Illinois