(UroToday.com) Upper tract urothelial carcinoma (UTUC) is associated with a poor prognosis despite radical nephroureterectomy. Similar to urothelial carcinoma of the bladder, outcomes are improved with perioperative platinum-based chemotherapy. Also similar to other urothelial cancers not all patients are eligible for platinum-based chemotherapy, often due to renal insufficiency, performance status, or antecedent neuropathy. These “cisplatin-ineligible” patients currently do not have the opportunity within standards of care to receive neoadjuvant systemic therapy. Prior attempts of single agent neoadjuvant pembrolizumab have been unsuccessful in unselected patients (PURE-02)1.
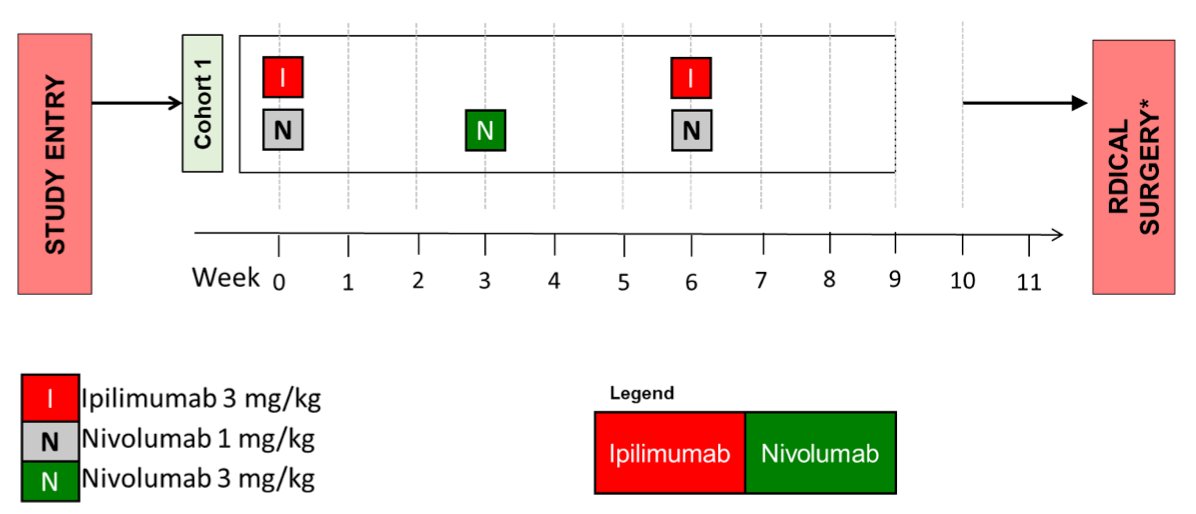
Here Dr. Min Yuen Teo and colleagues report the results from stage 1 of a phase II trial of neoadjuvant nivolumab and ipilimumab for UTUC. Key eligibility criteria included cisplatin-ineligibility and histologically confirmed high grade UTUC and/or evidence of radiographically-invasive disease with positive selective urine cytology. Treatment schema included doses of ipilimumab (3 mg/kg) and nivolumab (1 mg/kg) at weeks 0 and 6, with a dose of nivolumab (3 mg/kg) at week 3, followed by radical nephroureterectomy.
The primary endpoint was pathologic complete response (pCR) and secondary endpoints included pathologic downstaging (<tpT2N0), disease-free survival (DFS), and toxicity. The study employed a Simon optimal two-stage design with a total sample size of 24 patients by which if ≥1 of the initial 9 patients achieved a pCR in stage 1, the trial would proceed to accrue the total 24 patients.
In completion of stage 1, 9 patients were enrolled between 2/2021 and 7/2022 with median age 71 (range 62-86), of whom 89% (8/9) were male. Primary sites included ureter (n=6), renal pelvis (n=2), and both (n=1). Four patients (44%) had hydronephrosis and median tumor diameter was 3.0 cm, (range: not measurable to 4.2 cm). Six of 9 patients received all planned doses of systemic treatment. The three patients who did not complete systemic therapy were discontinued due to toxicity including diarrhea (grade 3), pneumonitis (grade 3), and one patient with grade 2 diarrhea, hyperthyroidism, and adrenal insufficiency. All patients underwent surgical resection at a median time of 1.7 months (range 0.6-3.7) following last systemic treatment. Two patients had metastatic progression (at 10.3, and 15.6 months) and two patient have died, one from post-operative sepsis and one from an unrelated fall.
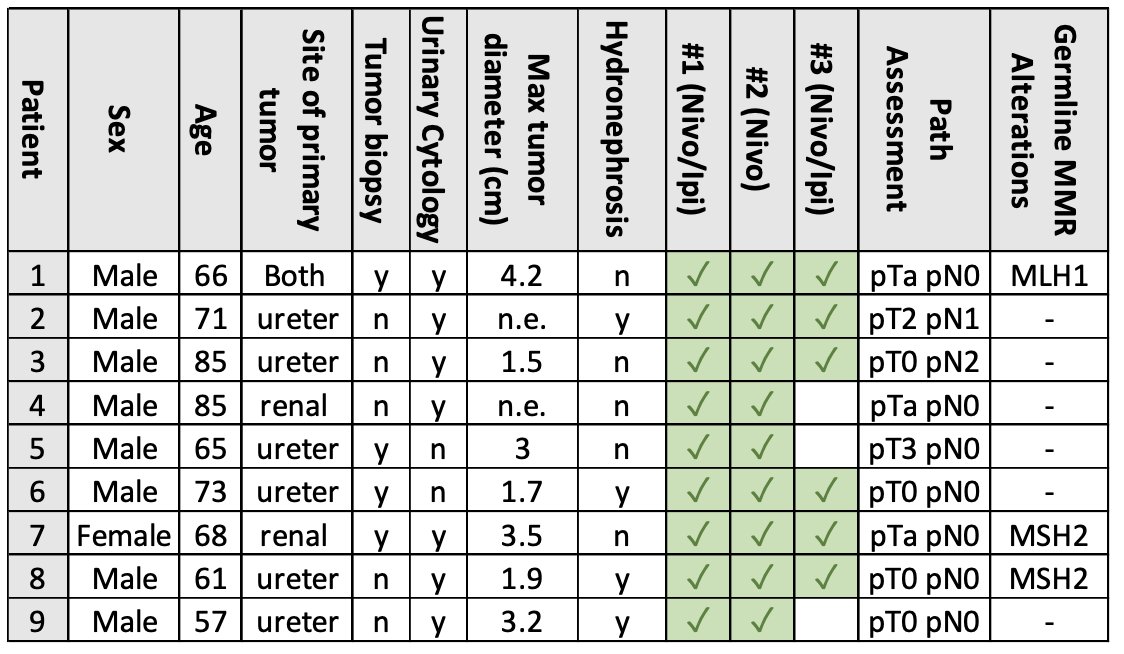
Three of 9 patients had a pCR and the remainder (6) achieved <ypT2pN0, consistent with pathological downgrading. Seven of 9 patients had pre-treatment sequencing via MSK-IMPACT with median tumor mutational burden (TMB) of 13.2 mutations/megabase (range 6.6-106.3). Among these, the three patients with TMB <10 Mt/MB were >ypT1 or node positive at surgery. In contrast, the four patients with TMB>10 all were <ypT1pN0. Pathogenic germline variants in genes mediating mismatch repair were identified in three patients (MLH1, MSH2), all of whom achieved either pCR (n=1) or ypTaN0 (n=2), and remain alive and disease-free at last follow up. No new safety signals were observed.

Dr. Teo concludes by highlighting the encouraging data of pathological responses with an absence of apparent unexpected safety signal in these patients who otherwise do not have an acceptable neoadjuvant standard of care prior to nephroureterectomy. The presence of genomic alterations conferring MMR deficiency highlights the relevance of patient selection when selecting therapies. Enrollment in stage 2 of the study is underway.
Presented by: Min Yuen Teo, MD, MRCP, Memorial Sloan Kettering Cancer Center
Written by: Jones Nauseef, MD, PhD, Assistant Professor of Medicine within the Division of Hematology and Medical Oncology, Sandra and Edward Meyer Cancer Center, and Englander Institute for Precision Medicine Weill Cornell Medicine and Assistant Attending physician at NewYork-Presbyterian Hospital. @DrJonesNauseef on Twitter during the 2023 American Society of Clinical Oncology Genitourinary (ASCO GU) Cancers Symposium, Thursday Feb 16 – Saturday Feb 18, 20223
- Necchi A, Martini A, Raggi D, Cucchiara V, Colecchia M, Lucianò R, Villa L, Mazzone E, Basile G, Scuderi S, Pederzoli F, Bandini M, Barletta F, Larcher A, Capitanio U, Salonia A, Briganti A, Ross JS, Messina A, Montorsi F. A feasibility study of preoperative pembrolizumab before radical nephroureterectomy in patients with high-risk, upper tract urothelial carcinoma: PURE-02. Urol Oncol. 2022 Jan;40(1):10.e1-10.e6. doi: 10.1016/j.urolonc.2021.05.014. Epub 2021 Jun 17. PMID: 34147313.
Neoadjuvant Nivolumab and Ipilimumab for Upper Tract Urothelial Cancer - Min Yuen Teo