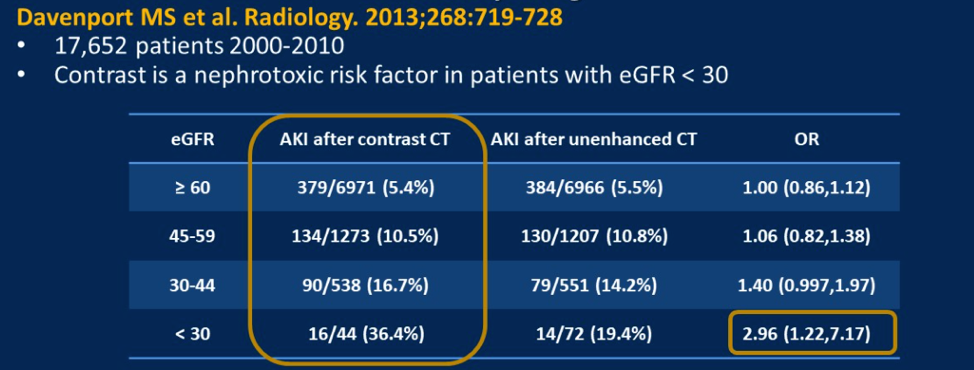
Regarding the risk of acute kidney injury with IV contrast, Dr. Potretzke highlighted two studies analyzing the incidence of AKI in large series of CT scans. One of the studies did not identify a clear difference in AKI risk with elevated creatinine, but another did. The clear findings from these studies are that the risk of AKI was not notably different at higher eGFR, but there is likely some risk when eGFR < 30. The numbers of patients included in the study that showed a higher odds ratio for AKI with contrast were relatively small, as seen below.

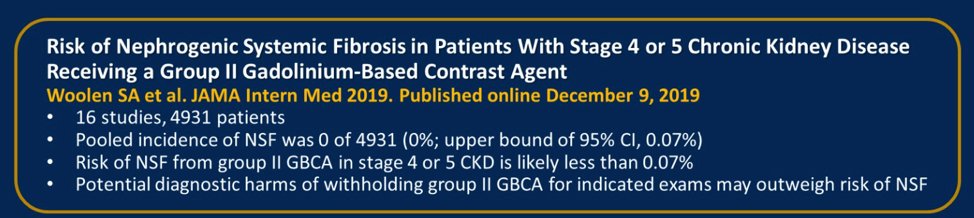
Switching to MRI, she then discussed that the type of gadolinium-based contrast agent (GBCA) is key to understanding the risk of nephrogenic systemic fibrosis (NSF). Group 1 agents, including Omniscan – gadodiamide, Magnevist (gadopentetate dimeglumine), and OptiMARK (Gadoversetamide) are associated with more than 99% of cases of single contrast agent NSF. Group 2 agents include MultiHance (gadobenate dimeglumine), Gadavist (Gadobutrol), Dotarem (gadoterate acid), and ProHance (gadoteridol). There is limited data on the group 3 agent Eovist (gadoxetate disodium). In one study of 4931 patients, the incidence of NSF was zero in patients administered group 2 GBCA, and thus kidney function screening is not mandatory. Group 1 GBCAs remain contraindicated if the patient is on dialysis, has acute kidney injury, or an eGFR < 30.
Finally, Dr. Potretzke discussed scan decision-making for a patient with eGFR < 30 either with or without acute kidney injury. She suggested that for a patient that is anuric with no change of renal recovery or on chronic dialysis, CT with contrast is a reasonable approach. However, if they are making urine and have a chance for renal recovery, then MRI with a class 2 GBCA is preferred.
Presented by: Theodora Potretzke, MD, Mayo Cinic, Rochester, Minnesota
Written by: Alok Tewari, MD, PhD, Medical Oncologist at the Dana-Farber Cancer Institute, during the 2021 American Society of Clinical Oncology Genitourinary Cancers Symposium (#GU21), February 11th-February 13th, 2021
References:
- Davenport M, Perazella M, Yee J et al. "Use of Intravenous Iodinated Contrast Media in Patients with Kidney Disease: Consensus Statements from the American College of Radiology and the National Kidney Foundation." Radiology. 2020. 10.1148/radiol.2019192094.
- Weinreb J, Rodby R, Yee J et al. "Use of Intravenous Gadolinium-based Contrast Media in Patients with Kidney Disease: Consensus Statements from the American College of Radiology and the National Kidney Foundation." Radiology. 2020. 10.1148/radiol.2020202903.