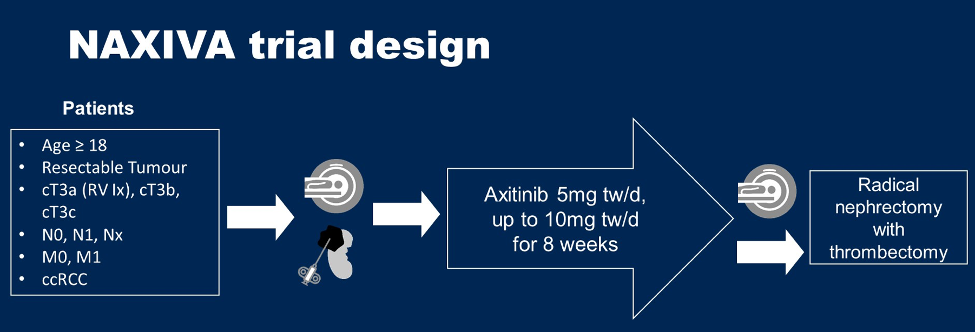
NAXIVA was a single-arm, single agent, multi-center Phase II feasibility study of axitinib in patients with both metastatic and non-metastatic clear cell RCC prior to nephrectomy and thrombectomy. A Simon two stage minimax design was adopted and the trial designed for adequate power to distinguish a <5% from a >25% improvement in the Mayo venous tumor thrombus level. There were 21 patients recruited over a 24-month period between December 15, 2017, and January 6, 2020, at five sites across the UK. Patients were treated with 8 weeks of axitinib (starting dose 5mg twice daily [BD], increasing to 10mg BD as tolerated) prior to planned surgery. The trial design of NAXIVA is as follows:
The primary endpoint was the percentage of evaluable patients with an improvement in venous tumor thrombus according to the Mayo classification (assessed using MRI abdomen scans at screening and week 9, prior to surgery). Secondary endpoints were percentage change in surgical approach, percentage change in venous tumor thrombus height, response rate (by RECIST), and evaluation of surgical morbidity assessed by Clavien-Dindo classification.
Among the 21 patients enrolled, 15 were male and the median age was 69 years old. There were 11 patients that were M0 and 10 M1 patients. The percentage of evaluable patients with an improvement in venous tumor thrombus according to the Mayo classification was 31.3% (80% confidence interval [CI] 19.6%-44.8%):
Ultimately, 17 patients proceeded to surgery of which 7 (41.1%) had a change in surgical approach to a less invasive option. There was a median percentage reduction in venous tumor thrombus height observed in 5 out of 17 patients (29.4%), and no patients had deterioration in “level of control” of the inferior vena cava (IVC)/renal vein. In terms of surgical morbidity, 11.7% (2 of 17 patients who progressed to surgery) experienced a Clavien-Dindo 3 or greater complication (one CVA intraoperatively and the patient died – grade V, one cardiorespiratory arrest – grade IVa). The median dose of axitinib was 5.8 mg (range 3.1-8.0 mg), with a median duration of therapy of 54 days (range: 16-57 days). The most common grade 3-5 adverse events were hypertension (24%), and fatigue (10%).
Dr. Stewart concluded his presentation of the NAXIVA trial with the following statements:
- Axitinib was effective based on a 31% response rate and on 41% of patients having a reduced extent of surgery after 8 weeks of axitinib treatment, showing it was possible to use systemic therapy to downstage venous tumor thrombus and reduce the extent of surgery
- Axitinib was safe in that toxicity was comparable to previous axitinib studies, with no evidence of an increase in operative morbidity or mortality
- There were no perceived negatives associated with axitinib neoadjuvant treatment as there was no clinically relevant venous tumor thrombus progression
Presented by: Grant D. Stewart, MD, PhD, Professor of Surgical Oncology, Honorary Consultant Urological Surgeon, University of Cambridge, Cambridge, United Kingdom
Written by: Zachary Klaassen, MD, MSc, Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Augusta, Georgia, Twitter: @zklaassen_md during the 2021 American Society of Clinical Oncology Genitourinary Cancers Symposium (#GU21), February 11th-February 13th, 2021