San Francisco, CA (UroToday.com) The combination of PARP inhibitor and androgen receptor-targeted therapy (ART) may induce enhanced therapeutic sensitivity and in patients with metastatic castration-resistant prostate cancer (mCRPC). A subset of mCRPC patients harbor mutations in DNA damage repair (DDR) genes, including BRCA1/2, conferring sensitivity to PARP inhibitors via synthetic lethality. Niraparib is a highly selective PARP inhibitor with potent activity against PARP-1 and PARP-2 enzymes that has demonstrated clinical benefit in second-line mCRPC (GALAHAD study). This phase 1b study, BEDIVERE (NCT02924766), is a multi-center, open-label study of niraparib plus ART, either apalutamide (APA) or abiraterone acetate plus prednisone (AA-P), comprising a dose selection phase (Part 1) with assessment of pharmacokinetics and dose-limit toxicities (DLT) and a dose expansion phase (Part 2). Eligible patients had mCRPC with or without DDR alterations who had received at least 1 line of prior chemotherapy or ART and no prior treatment with PARP inhibitor.
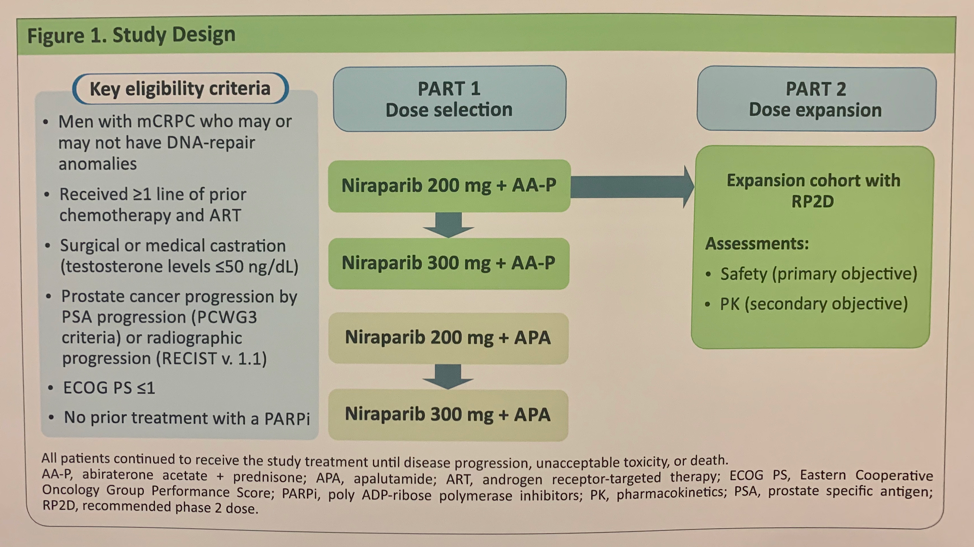
Results of the pharmacokinetic and DLT assessment of the niraparib plus APA combination demonstrated that at a dose of niraparib 200 mg, drug-drug interaction with APA led to low plasma drug levels. At a dose of niraparib 300 mg plus APA, 2 of 3 patients experienced a DLT, one with Grade 4 thrombocytopenia, the other with Grade 3 fatigue and hypertension. Given the pharmacokinetic and DLT results, the niraparib plus APA combination was discontinued.
The niraparib plus AA-P results were more promising. Four patients were treated with niraparib 200 mg plus AA-P with no DLTs. Three of 8 patients treated with niraparib 300 mg plus AA-P experienced DLTs: one with Grade 3 fatigue and Grade 4 elevated GGT, two with neutropenia. Thus, niraparib 200 mg was the recommended Phase 2 dose for combination with AA-P. This dose combination was evaluated in an additional 15 patients in Part 2. The median dose intensity for niraparib was 94.6% in the niraparib 200 mg cohort despite 14 of 19 patients experiencing at least 1 treatment-emergent adverse event (TEAE) leading to a dose interruption or reduction. Five of 19 patients in the niraparib 200 mg plus AA-P combination arm experienced at least one TEAE leading to discontinuation of study agents – these included nausea, vomiting, increased GGT, thrombocytopenia, and congestive heart failure. A summary of dose adjustments is outlined in the table below.
Below is a summary of the pharmacokinetics of niraparib after administration of 200 mg or 300 mg in combination with AA-P:

The authors concluded with the following take-home points:
- The combination of niraparib plus APA was not considered for further development due to DLTs associated with 300 mg and drug-drug interactions resulting in reduced exposure of niraparib
- Pharmacokinetic data suggest no drug-drug interactions between niraparib and AA-P
- The recommended Phase 2 dose for niraparib was 200 mg; no patients at this dose level experienced a DLT
- Niraparib 200 mg plus AA-P was well tolerated in a dose expansion cohort
- Based on the findings from this BEDIVERE study, the efficacy and safety of niraparib plus AA-P are being evaluated in the ongoing Phase 3 MAGNITUDE Study (NCT03748461)
Presented by: Fred Saad, MD, FRCS, Professor, Chief of Urology, and Director of GU Oncology, at the University of Montreal Hospital Center (CHUM), Montreal, Quebec, Canada
Written by: Jacob Berchuck, MD, Medical Oncology Fellow at the Dana-Farber Cancer Institute (Twitter: @jberchuck), at the 2020 ASCO Genitourinary Cancers Symposium (#GU20), February 13th to 15th, 2020, San Francisco, CA.