
Across a number of malignancies, PD-1/PD-L1 inhibitors promote a rapid, deep, durable response, including urothelial carcinoma, NSCLC, head and neck SCC, and colorectal cancer. Notably, much of this work was performed by Professors Jim Allison (MD Anderson Cancer Center) and Tasuku Honjo (Kyoto University), resulting in the Nobel Prize in Medicine in 2018. Much of what depicts whether a tumor will respond to immunotherapy portends from the tumor mutational burden: urothelial carcinoma has a high mutational burden and generally responds well, whereas prostate cancer does not and has historically responded poorly to immunotherapy. Further prognostication may be possible by assessing a tumor’s T-cell inflamed gene expression profile as a function of its tumor mutational burden.
With regards to bladder cancer, the Society of Immunotherapy of Cancer (SITC) developed a recent consensus statement on immunotherapy for bladder cancer1, with the following treatment algorithm:

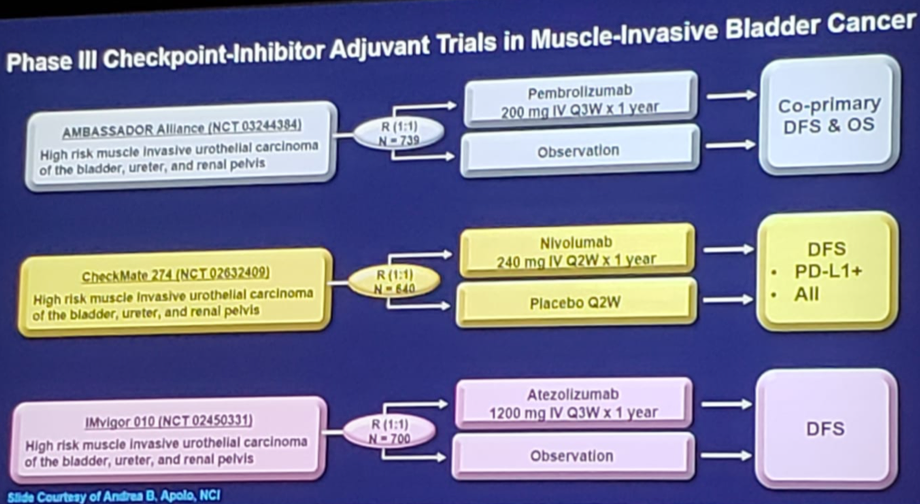
Dr. Gulley notes that across the major trials evaluating immunotherapy in bladder cancer (atezolizumab, nivolumab, pembrolizumab, avelumab, durvalumab) the objective response rate ranges from only 13.4-21.1%. One way to improve response for more patients are agents to elicit viral mimicry in the tumor tissue to potentiate and reinvigorate anti-tumor immunity; epigenetic reprogramming of T lymphocytes can overcome “immuno exhaustion”. One such study ongoing is testing atezolizumab + guadecitabine (a DNMTi) among patients with metastatic urothelial carcinoma that have progressed on prior checkpoint inhibitor therapy who still have measurable disease. As we have heard about at this meeting and several others in the last year or two, there are ongoing trials both in the adjuvant and neoadjuvant setting for bladder cancer:

Despite being an orphan disease, penile cancer has also recently been evaluated with regards to immunotherapy. As Dr. Gulley notes, it has been estimated that 63.3% of penile squamous cell carcinomas have been attributed to HPV infection, and over several small trials with HPV+ tumors, the objective response rate to PD-1/PD-L1 is in the range of 15-21%.
Similar to bladder cancer the SITC group has also published a consensus statement for renal cell carcinoma 2 with the following treatment algorithm:

Delving into the molecular biology, there is emerging work suggesting that endogenous retroviral signatures and CD8+ T-cell density may identify patients with mRCC who may respond to treatment. Dr. Gulley then highlighted the landmark CheckMate 214 study published last year3 in the New England Journal of Medicine. In this phase III trial, 1,096 patients were assigned to receive nivolumab plus ipilimumab (550 patients) or sunitinib (546 patients), including 425 and 422, respectively, that had intermediate or poor risk disease. At a median follow-up of 25.2 months in intermediate- and poor-risk patients, the 18-month overall survival rate was 75% with nivolumab plus ipilimumab and 60% with sunitinib. The median OS was not reached with nivolumab plus ipilimumab versus 26.0 months with sunitinib (HR for death 0.63; p <0.001). Furthermore, the objective response rate was 42% versus 27% (P<0.001), and the complete response rate was 9% versus 1%. The median PFS was 11.6 months (nivolumab + ipilimumab) and 8.4 months (sunitinib) (HR 0.82; p = 0.03, but significant per the prespecified 0.009 threshold).
The first-line immunotherapy disease space for mRCC is moving quickly. At ESMO 2018, the JAVELIN Renal 101 study presented initial results of this study in which patients were randomized to avelumab + axitinib vs sunitinib. The primary endpoint of PFS in the PD-L1+ group benefited avelumab + axitinib (HR 0.61, 95%CI 0.475-0.790), as did the key secondary endpoint of PFS in the overall population (HR 0.69, 95%CI 0.563-0.840; full report available). Dr. Gulley notes the results of the KEYNOTE-426 study coming soon also from ASCO GU 2019, assessing pembrolizumab + axitinib vs sunitinib in the first-line setting.
Dr. Gulley then discussed recent advances in prostate cancer and immunotherapy. He notes that pembrolizumab received FDA approval for MSI-high (MSI-H) mutation CRPC patients in 2017. A recent study from the Memorial Sloan Kettering Cancer Center assessed the prevalence of MSI-H/dMMR prostate cancer among 1,033 patients treated at their institution4, finding that 32 (3.1%) had MSI-H/dMMR disease. This included 23 patients (2.2%) that had tumors with high MSIsensor scores, and 7 of the 32 MSI-H/dMMR patients (21.9%) with a pathogenic germline mutation in a Lynch syndrome-associated gene. Eleven patients with MSI-H/dMMR CRPC received anti-PD-1/PD-L1 therapy and six of these had a greater than 50% decline in PSA levels. Based on these data, Dr. Gulley feels that every mCRPC patient should be tested.
The KEYNOTE-028 study was a trial of pembrolizumab in advanced solid tumors among patients with PD-1 expression ≥1% of tumor or stromal cells. Among 245 men screened, there were 35 PD-1% (14.3%) and 23 patients who enrolled5. There were four partial responses, for an objective response rate of 17.4% and 8 of 23 (34.8%) patients had stable disease. Median duration of response was 13.5 months, and median PFS and OS were 3.5 and 7.9 months, respectively. Furthermore, the 6-month PFS and OS rates were 34.8% and 73.4%, respectively. Dr. Gulley also touched on the results of the KEYNOTE-650 presented earlier during the GU ASCO ‘19 meeting testing nivolumab plus ipilimumab for treatment of mCRPC, details which can be found here:
Given the low tumor mutational burden for prostate cancer patients, Dr. Gulley notes that there is interest in vaccines as an integral component of immunotherapy for several reasons6:
- Engage an anti-tumor immune response
- Expand that immune response (eg. by cytokines, CTLA4)
- Enable effector function by reduction of immunosuppressive entities in the tumor microenvironment
- Bladder cancer – PD-L/PD-L1 inhibitors are approved in the second line, and first-line for cisplatin-ineligible patients. Investigations are ongoing in the first-line, adjuvant, neoadjuvant, and combination therapy
- Renal cancer – immunotherapy is approved in the second line (nivolumab) and first line (nivolumab + ipilimumab) and investigations are ongoing with PD-L/PD-L1 inhibitors in combination with VEGF inhibitors
- Prostate cancer – Sipuleucel-T is approved, as is pembrolizumab in MSI-H cancers and investigations are ongoing for combination immunotherapy
Presented by: James L. Gulley, The National Cancer Institute at the National Institute of Health, Bethesda, Maryland
Written By: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md at the 2019 American Society of Clinical Oncology Genitourinary Cancers Symposium, (ASCO GU) #GU19, February 14-16, 2019 - San Francisco, CA
References:
- Kamat AM, Bellmunt J, Galsky MD, et al. Society of Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of bladder carcinoma. J Immunother Cancer 2017 Aug 15;5(1):68
- Rini BI, McDermott DF, Hammers H, et al. Society of Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of renal cell carcinoma. J Immunother Cancer 2016 Nov 15;4:81
- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carinoma. N Engl J Med 2018;378(14):1277-1290.
- Abida W, Cheng ML, Armenia J, et al. Analysis of prevalence of microsatellite instability in prostate cancer and response to immune checkpoint blockade. JAMA Oncol 2018 Dec 27 [Epub ahead of print].
- Hansen AR, Massard C, Ott PA, et al. Pembrolizumab for advanced prostate adenocarcinoma: findings of the KEYNOTE-028 study. Ann Oncol 2018 Aug 1;29(8):1807-1813.
- Schlom J, Gulley JL. Vaccines as an Integral Component of Cancer Immunotherapy. JAMA 2018 Dec 4;320(21):2195-2196.