(UroToday.com) The 2026 ASCO annual meeting featured a radioligand innovation in prostate cancer session and a presentation by Dr. Renu Eapen discussing where we are now and where we are going. Dr. Eapen began her presentation by revisiting the origins of modern PSMA radioligand therapy.
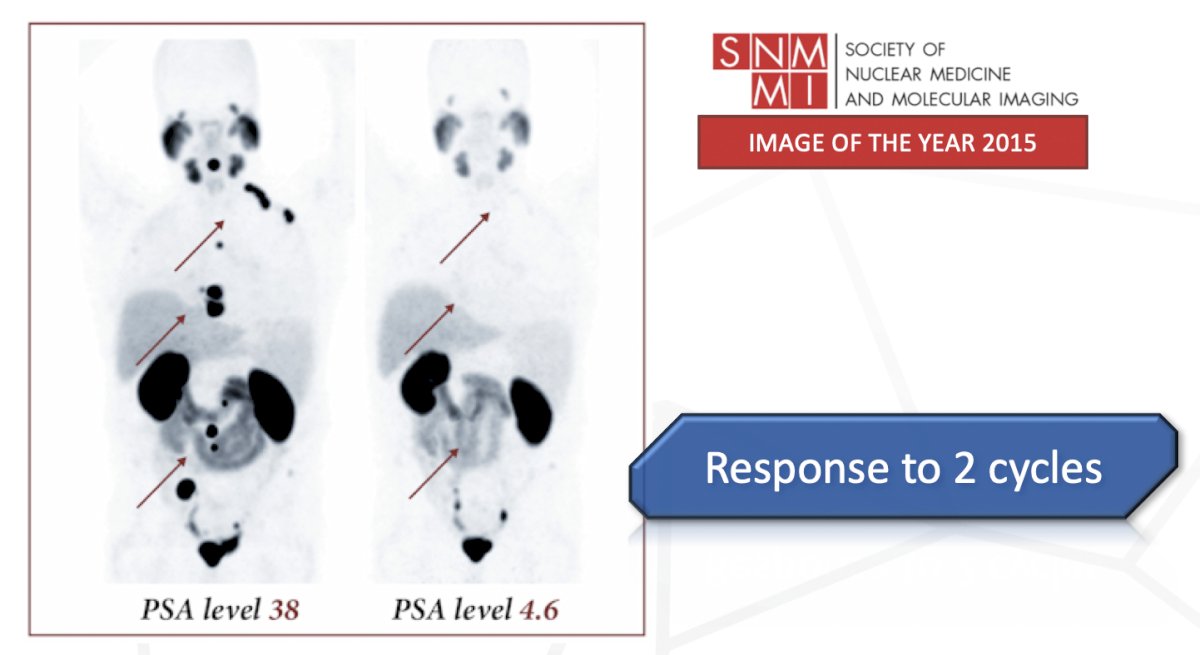
In 2015, Kratochwil and colleagues1 reported some of the first clinical experience with 177Lu-PSMA-617, demonstrating responses in heavily pretreated patients with metastatic castration-resistant prostate cancer (mCRPC). Early images presented during those initial reports highlighted profound reductions in tumor burden after only two cycles of therapy, helping establish the foundation for subsequent clinical development:
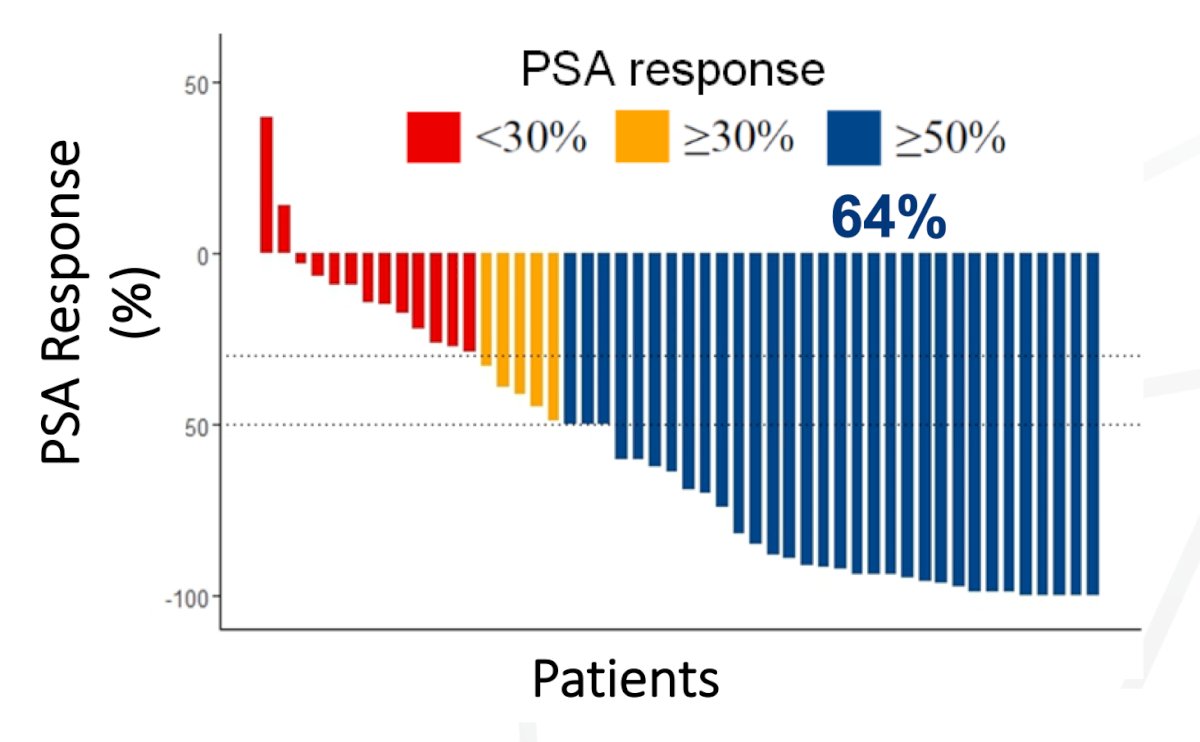
Dr. Eapen noted that one of the most influential early datasets came from the prospective phase 2 LuPSMA trial was only 50 patients.2 Despite the relatively small cohort, the study demonstrated a PSA response rate of 64% to 177Lu-PSMA-617, with these responses among patients who had exhausted conventional treatment options:
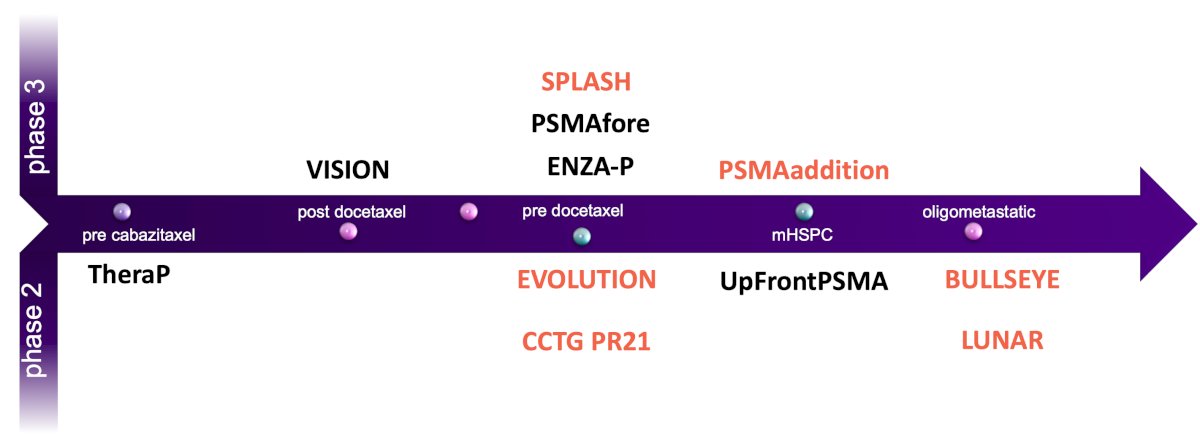
These findings ultimately contributed to the development of future trials. Dr. Eapen noted the studies that shaped the modern radioligand therapy landscape, including TheraP,3 VISION,4 ENZA-P,5 PSMAfore,6 and UpFrontPSMA.7 TheraP and VISION evaluated radioligand therapy in patients who had previously received docetaxel, whereas PSMAfore moved treatment earlier into the pre-docetaxel setting. UpFrontPSMA extended the concept even further into metastatic hormone-sensitive prostate cancer (mHSPC). By 2024, these studies had firmly established radioligand therapy as an effective treatment strategy across multiple disease states:
![These findings ultimately contributed to the development of future trials. Dr. Eapen noted the studies that shaped the modern radioligand therapy landscape, including TheraP [3], VISION [4], ENZA-P [5], PSMAfore,6 and UpFrontPSMA.7 TheraP and VISION evaluated radioligand therapy in patients who had previously received docetaxel, whereas PSMAfore moved treatment earlier into the pre-docetaxel setting. UpFrontPSMA extended the concept even further into metastatic hormone-sensitive prostate cancer (mHSPC). By 2024, these studies had firmly established radioligand therapy as an effective treatment strategy across multiple disease states:](/images/com-doc-importer/271-asco-2026/asco-2026-radioligand-revolutions-where-we-are-now-and-where-we-are-going/image-2.jpg)
Looking ahead to 2026, the radioligand therapy landscape continues to expand. Dr. Eapen highlighted several ongoing and emerging studies, including PSMAddition, SPLASH, EVOLUTION, BULLSEYE, LUNAR,8 and CCTG PR21:
These trials are evaluating radioligand therapy across a broad spectrum of disease states, including oligometastatic disease, hormone-sensitive disease, and earlier lines of metastatic castration-resistant disease.
Dr. Eapen then presented a conceptual framework illustrating how radioligand therapy has steadily migrated earlier in the prostate cancer disease continuum. Historically, radioligand therapy occupied a late-line position following ARPI, chemotherapy, and progression to symptomatic mCRPC. However, emerging data from PSMAfore, ENZA-P, UpFrontPSMA, PSMAaddition, and other studies suggest that radioligand therapy may continue moving toward earlier stages of disease management:

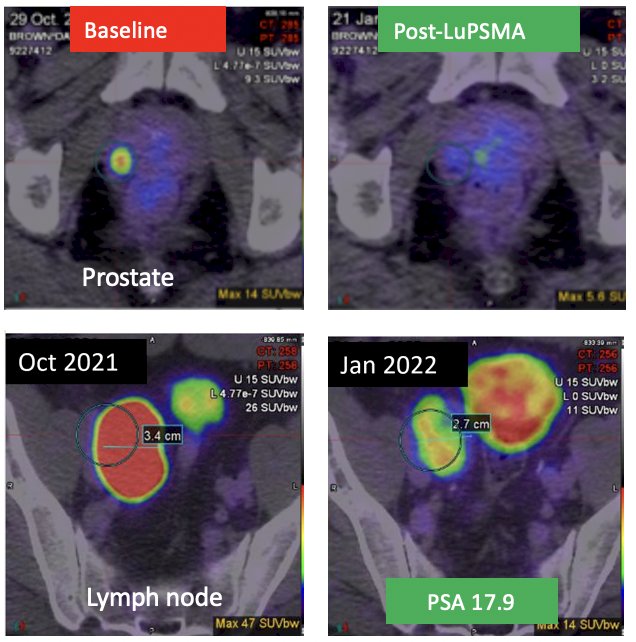
LuTectomy9 is an innovative neoadjuvant radioligand therapy approach being evaluated before radical prostatectomy. Dr. Eapen highlighted the experience of a 62-year-old man who initially presented with a PSA of 334 ng/mL, clinical stage cT1c disease, PIRADS 2 findings, Grade Group 1 disease, cN1 lymph node involvement, and a PSMA PET SUVmax of 47. Following a 177Lu-PSMA-617 cycle of treatment, his PSA declined to 17.9 ng/mL, and he subsequently underwent a robotic radical prostatectomy, which demonstrated pT3a Grade Group 4 disease with negative surgical margins and pathologic nodal involvement (pN1). Most notably, the patient maintained a PSA <0.2 ng/mL at 18 months of follow-up:
Data from the Peter MacCallum phase I/II program suggest that 177Lu-PSMA-617 may induce an immunogenic response, potentially creating opportunities for combination approaches with immunotherapy. Dr. Eapen emphasized that the ability of radioligand therapy to modify the tumor microenvironment may represent an important mechanism underlying future therapeutic combinations.
The second half of the presentation focused on future directions for radioligand therapy development, organized around three major themes: new targets, new isotopes, and combination therapies. With regard to new targets, Dr. Eapen noted that PSMA will likely remain important, but numerous additional targets are now under active investigation. These include ACP3, STEAP1/2, B7-H3, hK2, GRPR, DLL3, SSTR2, FAP, PARP-related targets, and CD46:
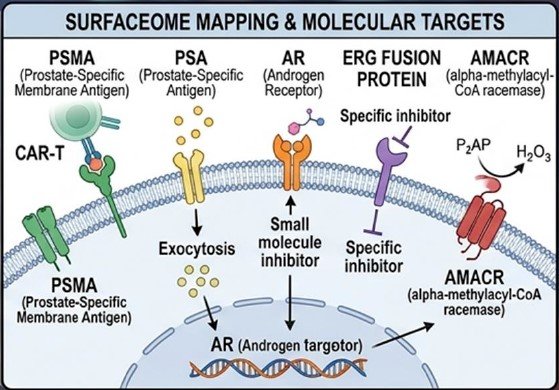
Many of these targets offer distinct advantages, including expression in aggressive disease phenotypes, lower salivary gland uptake, reduced renal uptake, and activity in tumors with limited PSMA expression.
ACP3 (prostatic acid phosphatase) is one of the most promising emerging targets, demonstrating near-universal expression in more than 95% of prostate cancers and exhibiting a favorable biodistribution profile. Current radiopharmaceuticals under development include 68Ga-OncoACP3-DOTA for PET imaging, 177Lu-OncoACP3, and 225Ac-OncoACP3. Importantly, ACP3 may be particularly relevant in aggressive neuroendocrine and dedifferentiated prostate cancers that have lost PSMA expression. Lower salivary gland and renal uptake could potentially reduce xerostomia and nephrotoxicity. However, Dr. Eapen cautioned that only very early human data are currently available, and efficacy and survival outcomes remain unknown.
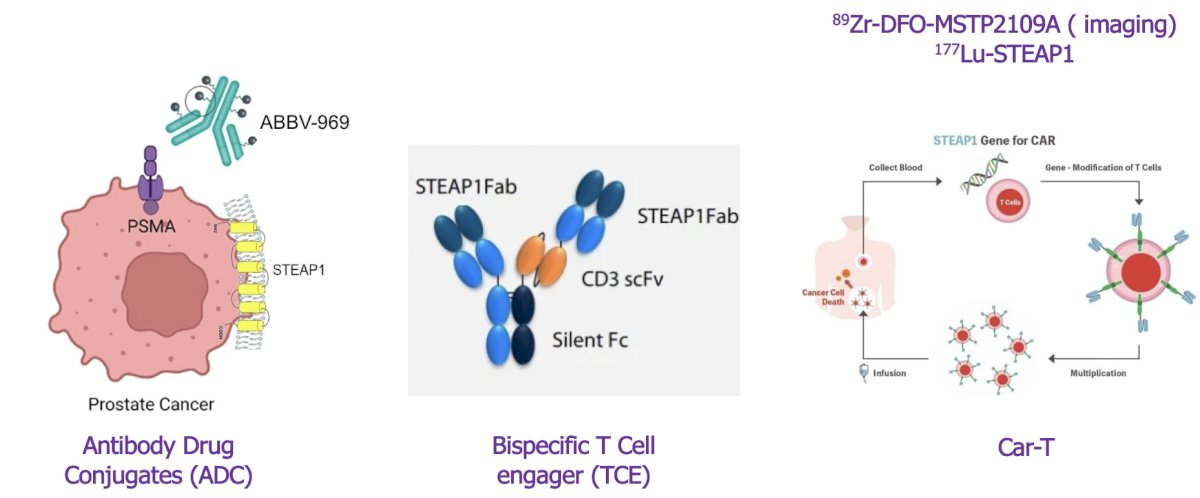
STEAP1 and STEAP2 are cell surface metalloreductases, demonstrating high prostate specificity and are strongly expressed in prostate cancer. Multiple therapeutic approaches are under development, including antibody drug conjugates, bispecific T-cell engagers, CAR-T cell therapies, imaging agents such as 89Zr-DFO-MSTP2109A, and radioligand therapies including 177Lu-STEAP1. Their near-universal expression and virtual absence in salivary glands and kidneys make them particularly appealing candidates for future development:
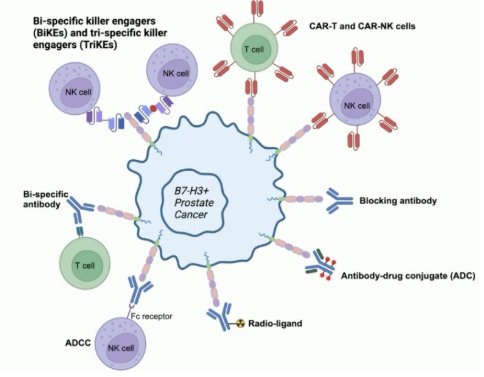
Another exciting target is B7-H3, a protein that is overexpressed in aggressive disease states and has been associated with metastasis, androgen independence, and poor prognosis. Importantly, B7-H3 may play a role in PSMA-non-avid tumors and therefore represents a potential strategy for overcoming resistance to PSMA-directed therapy. Dr. Eapen described B7-H3 as one of the hottest emerging radioligand targets in solid tumors and suggested that it could ultimately become a leading target for aggressive and PSMA-resistant prostate cancer phenotypes:
Turning to isotopes, Dr. Eapen highlighted ongoing efforts involving actinium, lead, copper, and terbium:
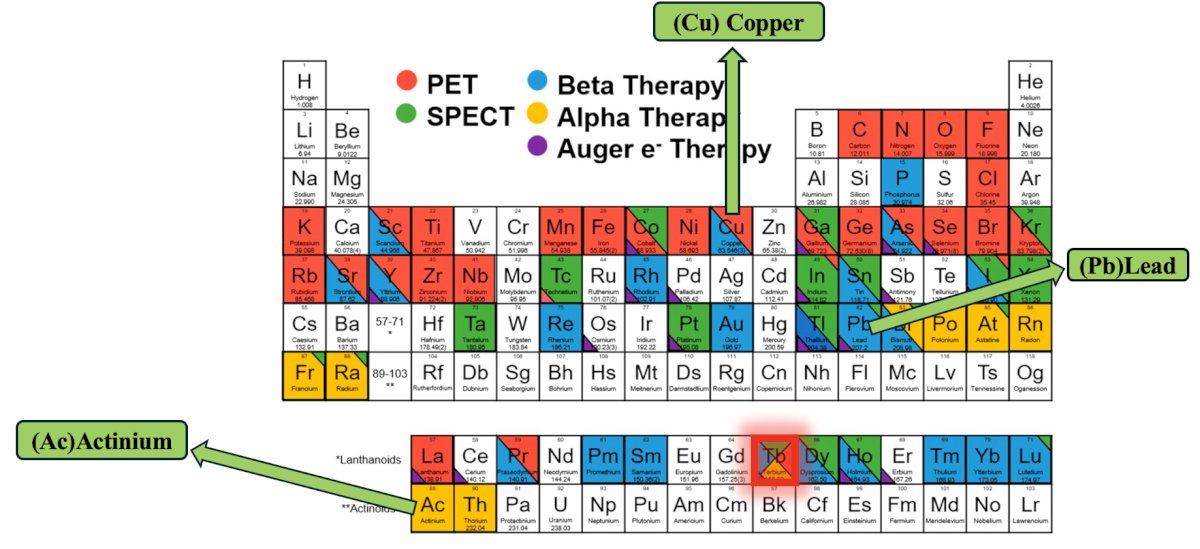
The first in-human trial of 161Tb-PSMA demonstrated deep PSA responses, with PSA reductions of at least 90% observed in 40% of patients (12 of 30 treated patients).10 Treatment was delivered at 7.4 GBq and was associated with a favorable safety profile. Because terbium emits both beta particles and Auger/conversion electrons, it may be particularly effective against micrometastatic disease while maintaining encouraging clinical activity.
Finally, Dr. Eapen reviewed a growing number of studies combining 177Lu-PSMA with other treatment modalities. These include:
- Immunotherapy combinations such as PRINCE (pembrolizumab) and EVOLUTION (ipilimumab + nivolumab)
- Hormonal therapy combinations such as ENZA-p
- Chemotherapy combinations including UpFrontPSMA and LuCAB
- PARP inhibitor combinations such as Lu-PARP with olaparib
- Bone-targeted combinations such as AlphaBET utilizing radium-223
- Surgical approaches, including LuTectomy
- Radiation-based strategies such as POPSTAR 2
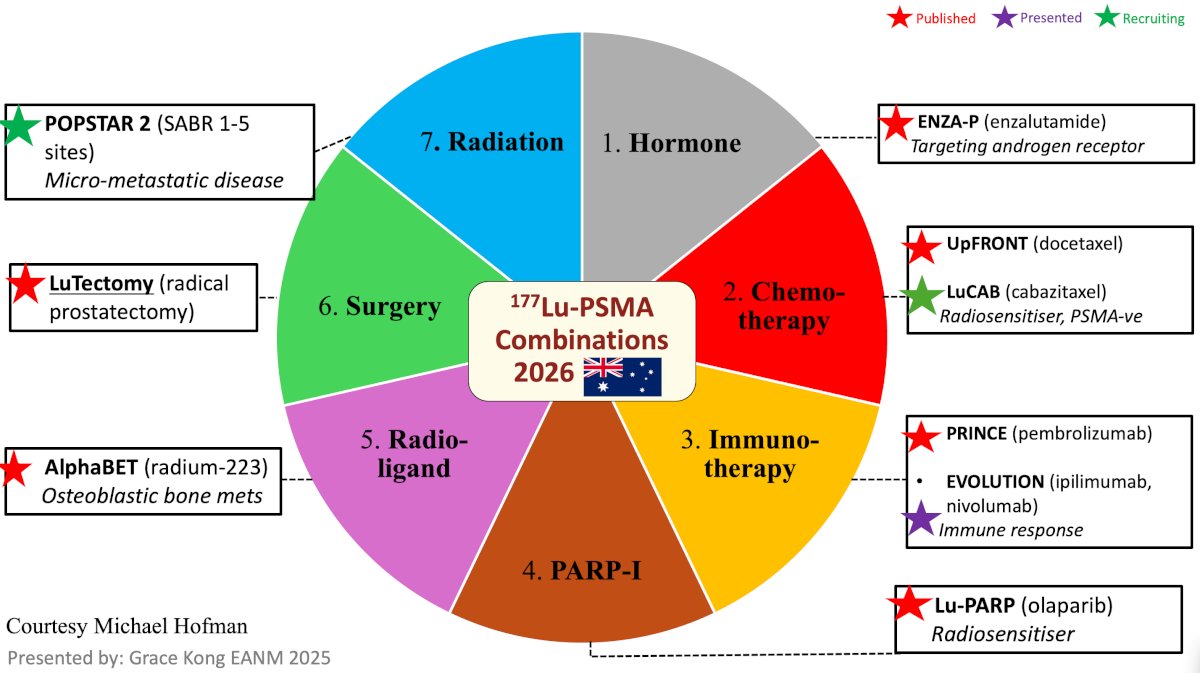
Many of these studies are moving radioligand therapy into earlier stages of disease rather than reserving it exclusively for mCRPC. Second, several combination studies have already generated published results, while numerous others are actively recruiting or have recently reported encouraging preliminary findings.
Presented by: Renu Eapen, MBBS, FRACS, Peter MacCallum Cancer Centre, Melbourne, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:
- Kratochwil C, Giesel FL, Eder M, et al. [177Lu]Lutetium-labelled PSMA ligand-induced remission in a patient with metastatic prostate cancer. Eur J Nucl Med Mol Imaging. 2015 May;42(6):987-988.
- Hofman MS, Violet J, Hicks RJ, et al. [177Lu]-PSMA-617 radionuclide treatment in patients with metastatic castration-resistant prostate cancer (LuPSMA trial): A single-center, single-arm phase 2 study. Lancet Oncol 2018 Jun;19(6):825-833.
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Emmett L, Subramaniam S, Crumbaker M, et a. [177Lu]Lu-PSMA-617 plus enzalutamide in patients with metastatic castration-resistant prostate cancer (ENZA-p): An open-label, multicentre, randomized, phase 2 trial. Lancet Oncol. 2024 May;25(5):563-571.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Azad AA, Bressel M, Tan H, et al. Sequential [(177)Lu]Lu-PSMA-617 and docetaxel versus docetaxel in patients with metastatic hormone sensitive prostate cancer (UpFrontPSMA): A multicentre, open label, randomized, phase 2 study. Lancet Oncol. 2024 Oct;25(10):1267-1276.
- Kishan AU, Valle LF, Wilhalme H, et al. 177Lu-Prostate-Specific Membrane Antigen Neoadjuvant to Stereotactic Ablative Radiotherapy for Oligorecurrent Prostate Cancer (LUNAR): An open-label, randomized, controlled, phase II study. J Clin Oncol. 2025 Dec 20;43(36):3812-3821.
- Eapen RS, Buteau JP, Jackson P, et al. Administering [177Lu]Lu-PSMA-617 Prior to Radical Prostatectomy in Men with High-risk Localized Prostate Cancer (LuTectomy): A Single-centre, single-arm, phase 1/2 study. Eur Urol. 2023 Oct 25:S0302-2838(23)03087-7.
- Buteau JP, Kostos L, Jackson PA, et al. First-in-human results of terbium-161 [161Tb]Tb-PSMA-I&T dual beta-Auger radioligand therapy in patients with metastatic castration-resistant prostate cancer (VIOLET): A single-centre, single-arm, phase 1/2 study. Lancet Oncol. 2025 Aug;26(8):1009-1017.