(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL, was host to the Prostate, Testicular, and Penile Cancer - Oral Abstracts. Dr. Atish D. Choudhury presented Abstract 5004: A phase 2 trial of ADT interruption in patients responding exceptionally to androgen receptor pathway inhibitor in mHSPC (A-DREAM / Alliance A032101).
Dr. Choudhury began by discussing the rationale for moving forward with the A-DREAM study in the modern era of intensified systemic therapy for metastatic hormone-sensitive prostate cancer. He noted that prior randomized studies evaluating intermittent versus continuous androgen deprivation therapy demonstrated broadly comparable overall survival outcomes in some settings. However, in the metastatic (M1) population, the SWOG 9346 trial failed to demonstrate non-inferiority of intermittent therapy, reporting a hazard ratio for death of 1.10 (90% CI 0.99-1.23), which did not meet the prespecified non-inferiority margin.1
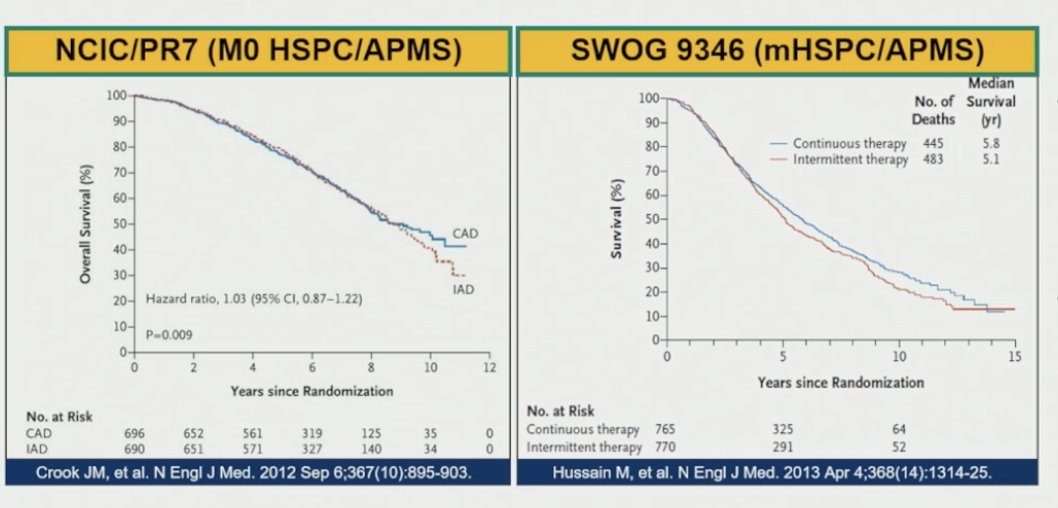
Importantly, he emphasized that these historical data must be interpreted cautiously in the contemporary treatment landscape. In SWOG 9346, patients discontinued ADT after only 7 months of therapy if PSA decreased to <4 ng/mL, with treatment resumed only after PSA increased to >20 ng/mL or above baseline levels. He highlighted that this approach differs substantially from current practice patterns, particularly given the incorporation of ARPIs, treatment intensification strategies, and modern imaging techniques, all of which provided the rationale for revisiting treatment de-escalation strategies within A-DREAM.
Dr. Choudhury then discussed what is currently known in the modern treatment era. He noted that the addition of potent androgen receptor pathway inhibitors to ADT deepens treatment responses and significantly prolongs survival in metastatic hormone-sensitive prostate cancer. However, he emphasized that continuous treatment with ADT plus ARPIs is associated with important cumulative toxicities extending beyond the short term, including bone loss, cardiovascular complications, metabolic changes, impaired quality of life, and substantial financial costs. Moreover, achieving a PSA <0.2 ng/mL with ADT plus ARPI therapy is consistently associated with highly favorable clinical outcomes.2
Based on these observations, the investigators hypothesized that prolonged treatment with ADT plus ARPI, rather than testosterone suppression alone, combined with selection of patients achieving the deepest responses, may permit safe treatment interruption while allowing testosterone recovery. This concept formed the basis for the A-DREAM study strategy evaluating treatment de-escalation in exceptional responders
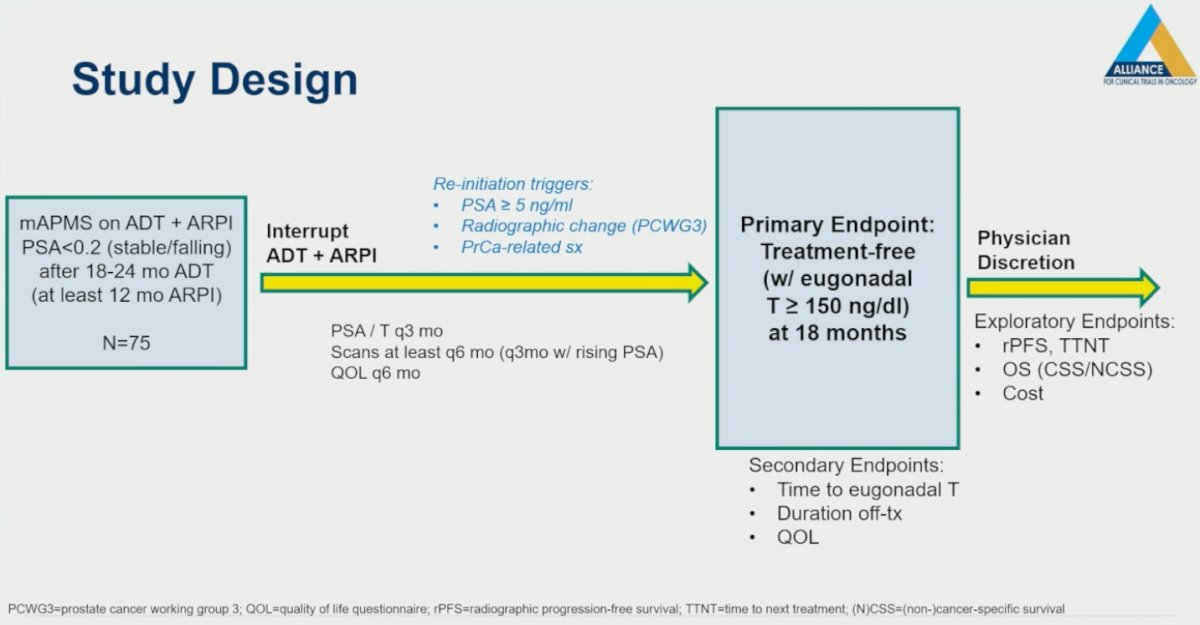
The A-DREAM study design was intentionally straightforward and focused on evaluating whether carefully selected patients with metastatic hormone-sensitive prostate cancer could safely interrupt systemic therapy after achieving an exceptional response. Eligible patients had metastatic disease treated with ADT plus an ARPI and were required to achieve a stable or falling PSA <0.2 ng/mL after 18–24 months of ADT, including at least 12 months of ARPI therapy. A total of 75 patients meeting these criteria subsequently underwent interruption of both ADT and ARPI treatment.
Following treatment interruption, patients were closely monitored with PSA and testosterone assessments every 3 months, surveillance imaging at least every 6 months, and quality-of-life evaluations every 6 months, with imaging performed more frequently in the setting of rising PSA levels. Treatment re-initiation was triggered by predefined criteria, including PSA ≥5 ng/mL, radiographic progression according to PCWG3 criteria, or development of prostate cancer-related symptoms. The primary endpoint of the study was treatment-free survival with eugonadal testosterone recovery, defined as testosterone ≥150 ng/dL, at 18 months. Secondary endpoints included time to eugonadal testosterone recovery, duration off therapy, and quality-of-life outcomes. Beyond study primary endpoint timeline (18 months), all subsequent management decisions were left to physician discretion. The study design is shown below:
The statistical design was structured around the key clinical question of whether a meaningful proportion of patients could remain treatment-free with testosterone recovery at 18 months. The study was powered to distinguish an 18-month treatment-free rate of 30% under the null hypothesis from 45% under the alternative hypothesis. Patients who discontinued study participation after treatment interruption but before the 18-month assessment were conservatively counted as not remaining treatment-free. With 71 evaluable patients, the design provided a type I error rate of 0.10 and 90% power to detect an improvement from 30% to 45%. Anticipating approximately 5% dropout, including progression after enrollment or patient/physician decision not to discontinue therapy, the target accrual was set at 75 patients.
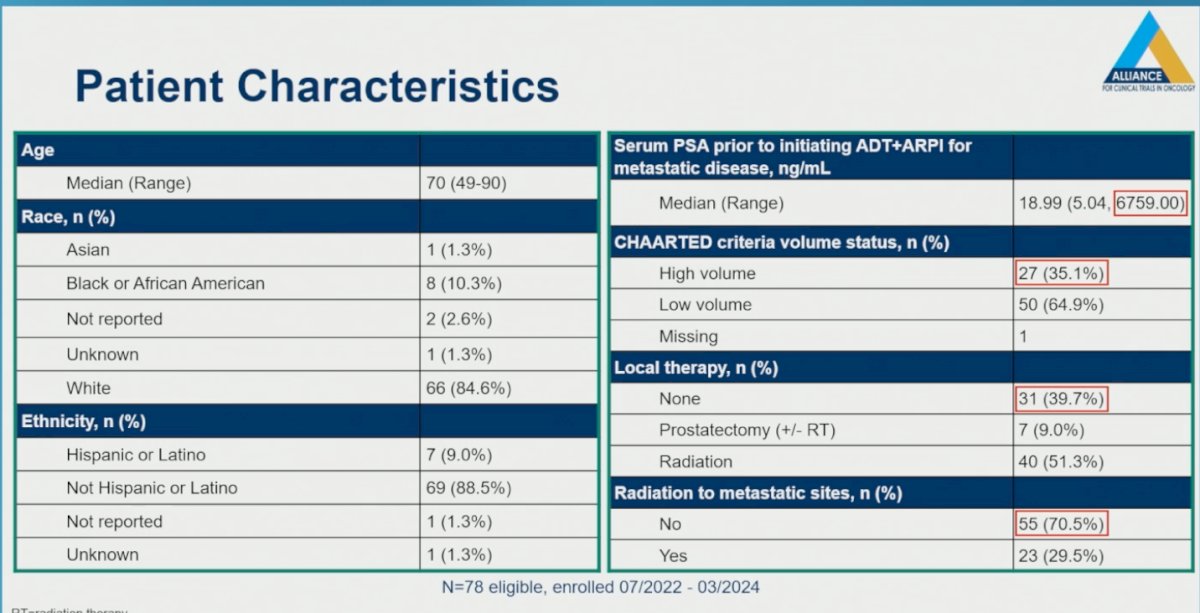
The cohort included a clinically heterogeneous population, with 35.1% of patients meeting CHAARTED high-volume disease criteria. Median PSA prior to initiation of ADT plus ARPI was 18.99 ng/mL, although values ranged widely from 5.04 to 6759.00 ng/mL, reflecting substantial variability in baseline disease burden. Additionally, 39.7% of patients had not received prior local therapy, while 29.5% had previously undergone radiation directed at metastatic sites as illustrated below:
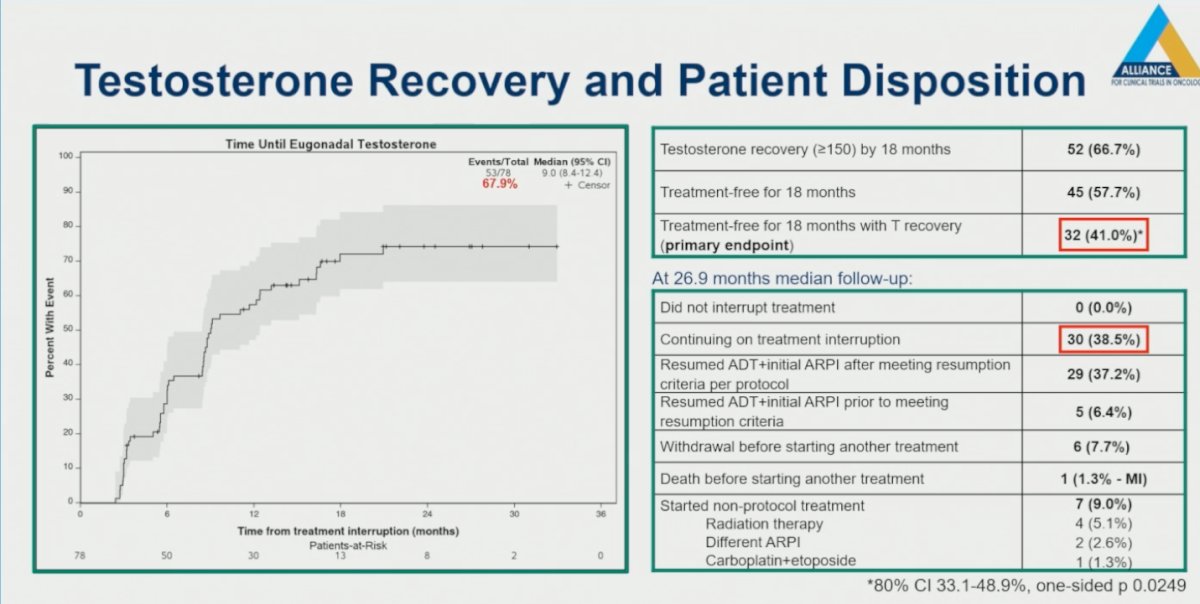
At 18 months following treatment interruption, 66.7% of patients achieved testosterone recovery to eugonadal levels (≥150 ng/dL), while 57.7% remained treatment-free. Importantly, 41.0% of patients met the primary endpoint of remaining treatment-free for 18 months while also achieving testosterone recovery. This result was statistically significant, meeting the predefined study endpoint threshold (80% CI 33.1–48.9%; one-sided p=0.0249).
At a median follow-up of 26.9 months, 38.5% of patients remained on treatment interruption without requiring re-initiation of therapy, suggesting that a meaningful proportion of exceptional responders were able to sustain prolonged treatment-free intervals. Overall, 37.2% of patients resumed ADT plus initial ARPI therapy after meeting predefined protocol resumption criteria, while an additional 6.4% restarted treatment prior to formally meeting those criteria. Importantly, one patient developed neuroendocrine progression and subsequently required carboplatin plus etoposide chemotherapy. Additionally, 9.0% of patients initiated non-protocol therapies, including radiation therapy, a different ARPI, or platinum-based chemotherapy.
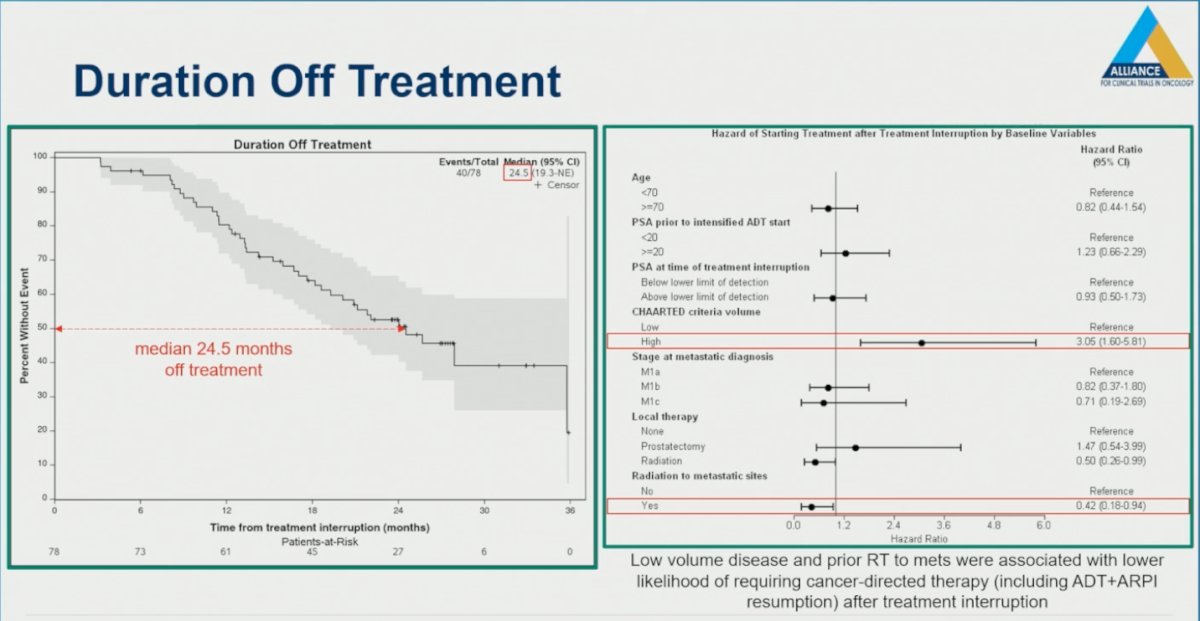
The median duration off treatment was 24.5 months, substantially longer than initially anticipated, supporting the feasibility of prolonged treatment interruption in selected patients with exceptional responses to ADT plus ARPI therapy. The investigators also explored baseline clinical factors associated with the likelihood of requiring re-initiation of cancer-directed therapy following treatment interruption. Notably, patients with CHAARTED high-volume disease were significantly more likely to require treatment resumption after interruption (HR 3.05, 95% CI 1.60-5.81). In contrast, patients who had previously received radiation therapy directed at metastatic sites were less likely to require re-initiation of systemic therapy following interruption (HR 0.42, 95% CI 0.18-0.94).
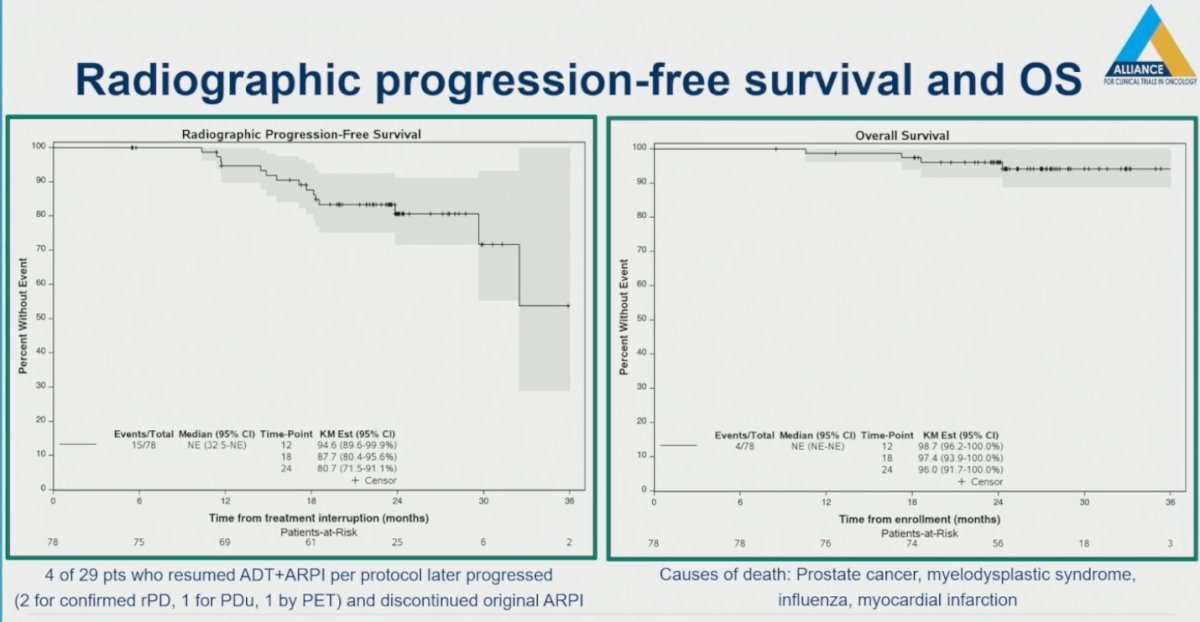
Radiographic progression-free survival and overall survival outcomes remained favorable despite treatment interruption. Importantly, the investigators highlighted that radiographic progression while off therapy did not necessarily indicate permanent loss of benefit from prior ARPI treatment. Among the 29 patients who resumed ADT plus ARPI per protocol, only 4 subsequently progressed, including 2 patients with confirmed radiographic progression, 1 with PSA progression, and 1 progression detected by PET imaging, suggesting that many patients were able to regain disease control following treatment re-initiation.
Overall survival outcomes also remained encouraging during follow-up. There were 4 deaths reported in the study, with causes of death including prostate cancer, myelodysplastic syndrome, influenza, and myocardial infarction, underscoring the importance of competing comorbidities and non-cancer-related events in this patient population.
Lastly, Dr. Choudhury acknowledged several important limitations of the A-DREAM study. He emphasized that this was a single-arm study without a comparator arm, limiting the interpretability of outcomes and making it difficult to definitively determine the long-term impact of treatment interruption strategies. He also highlighted the issue of patient selection, noting that the study inherently selected for patients and clinicians who were both willing and motivated to interrupt therapy, potentially introducing bias toward more favorable or highly engaged patients.
Additional limitations included the relatively small sample size and the still unclear relationship between the primary endpoint and long-term oncologic outcomes. He noted that only a limited number of radiographic progression-free survival and overall survival events had occurred thus far, with longer-term follow-up and quality-of-life analyses still pending. Protocol non-adherence was also observed and, to some extent, expected in this clinical setting, including patients restarting therapy prior to meeting protocol-defined resumption thresholds. Furthermore, some patients received off-protocol treatments, most commonly radiation therapy or switching to a different ARPI, which may further complicate interpretation of efficacy outcomes.
Dr. Choudhury concluded with the following key takeaway messages:
- A-DREAM/A032101 met its primary endpoint, with 41% of patients remaining treatment-free with testosterone recovery 18 months after interruption of ADT plus ARPI therapy.
- At a median follow-up of 26.9 months, 38.5% of patients remained on treatment interruption, suggesting that durable treatment-free intervals may be achievable in selected exceptional responders.
- Only 1 of the 4 deaths observed during the study was attributed to prostate cancer, highlighting the importance of competing risks and long-term treatment-related morbidity in this patient population.
- Although level I phase III data are not yet available in this setting, the investigators believe that, given the cumulative short- and long-term toxicities associated with continuous therapy, carefully selected treatment holidays represent a reasonable clinical consideration.
- Optimal intermittent treatment strategies still require further prospective study and refinement in the modern era of intensified systemic therapy.
Presented by: Atish D. Choudhury, MD, PhD, Medical Oncologist, Dana Farber Cancer Institute, Boston, MA
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on X during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026
References:- Hussain M, Tangen CM, Berry DL, Higano CS, Crawford ED, Liu G, Wilding G, Prescott S, Kanaga Sundaram S, Small EJ, Dawson NA, Donnelly BJ, Venner PM, Vaishampayan UN, Schellhammer PF, Quinn DI, Raghavan D, Ely B, Moinpour CM, Vogelzang NJ, Thompson IM Jr. Intermittent versus continuous androgen deprivation in prostate cancer. N Engl J Med. 2013 Apr 4;368(14):1314-25. doi: 10.1056/NEJMoa1212299. PMID: 23550669; PMCID: PMC3682658.
- Freedland SJ, Hong A, El-Chaar N, Murty S, Ramaswamy K, Coutinho AD, Nimke D, Morgans AK. Prostate-specific antigen response and clinical progression-free survival in Black and White men with chemotherapy-naïve metastatic castration-resistant prostate cancer treated with enzalutamide in a real-world setting. Prostate Cancer Prostatic Dis. 2023 Sep;26(3):523-530. doi: 10.1038/s41391-022-00622-6. Epub 2022 Dec 14. PMID: 36517634; PMCID: PMC10449620.