This has come as a result of the introduction of cisplatin-based chemotherapy in the 1970s.

However, studies have reported an increased risk of mortality among testis cancer survivors which has been felt to be due to the effects of platinum-based chemotherapy and radiotherapy. This is particularly notable at 20 years following diagnosis.

There are limitations to these analyses, including the completeness of data regarding chemotherapy exposure. In the Prostate, Testicular, and Penile Oral Abstract Session at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Dr. Ragnhild Hellesnes presented a population-based assessment of causes of death and mortality rates for patients with testicular cancer who were treated in the cisplatin era.
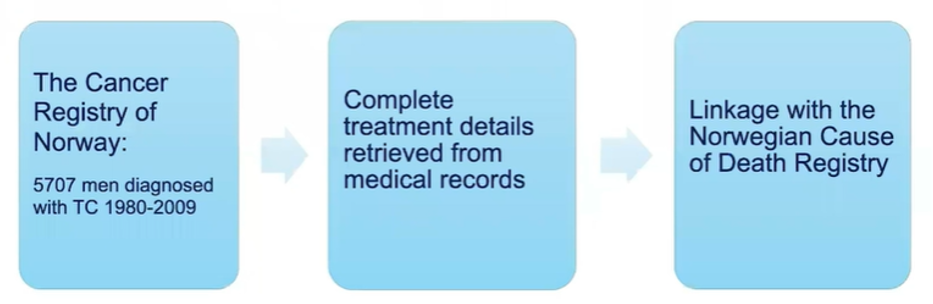
The authors identified 5,707 men diagnosed with testis cancer between 1980 and 2009 from the Cancer Registry of Norway. The authors restricted to men above age 16 years at diagnosis without a prior history of malignancy. They further excluded men with non-germ cell tumors. They extracted data regarding clinical parameters and treatment data from medical records and linked these data with the Norwegian Cause of Death Registry to ascertain the cause of death which was classified according to the European Shortlist.
The authors calculated standardized mortality ratios (SMRs) to compare the cause-specific mortality in the cohort to an age-matched general population. They also assess the absolute excess risks. Among patients undergoing chemotherapy, the authors calculated age-adjusted hazard ratios (HRs) to evaluate the association between the number of cycles of platinum-based chemotherapy on non-testis cancer mortality using time-based Cox regression models.
The authors followed these 5,707 men for a median of 18.7 years. Over this time, 665 (12%) men died of non-testis cancer causes. Overall, 25% of patients received surgery alone, 44% received platinum-based chemotherapy, 27% received radiotherapy, and 4% received a combination of chemotherapy and radiotherapy.

Among those who received chemotherapy, the preponderance received four or more cycles (57%).
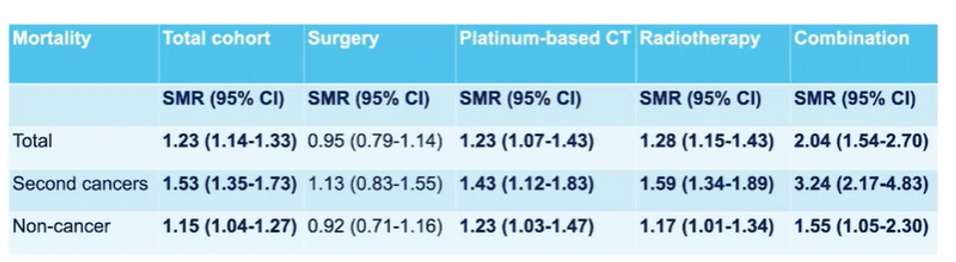
Compared to the general population, testis cancer survivals had an excess of non-testis cancer morality overall (SMR 1.23, 95% CI 1.14-1.33). When examined by treatment approach, patients who underwent surgery experienced no increased risk of mortality (SMR 0.95, 95% CI 0.79-1.14), though the risk was increased after both platinum-based chemotherapies (SMR 1.23, 95% CI 1.06-1.42) and radiotherapy (SMR 1.28, 95% CI 1.15-1.43).
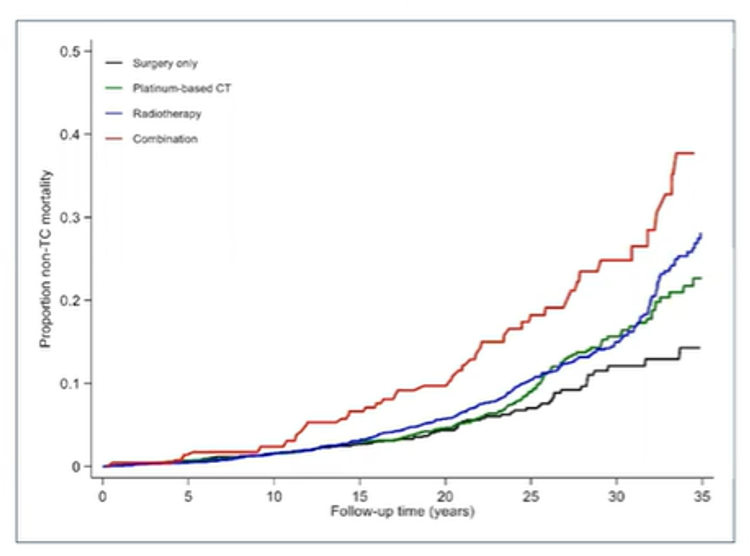
Visualized using cumulative incidence curves, a similar effect can be seen with an increased risk of non-testis cancer mortality for patients receiving chemotherapy, radiotherapy, or the combination of the two.
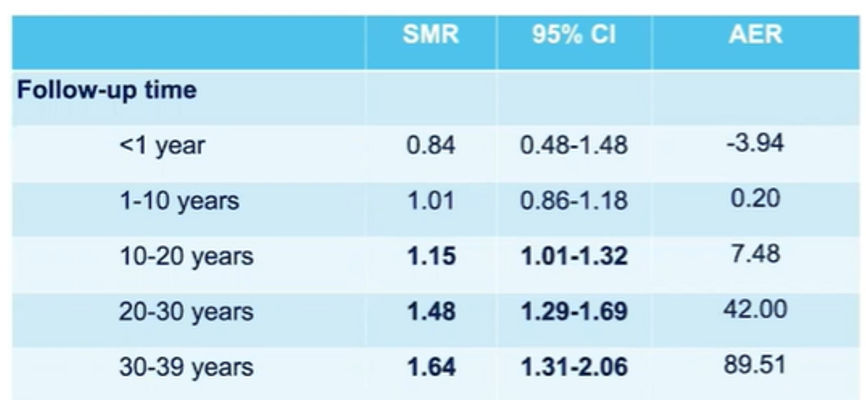
Further, as follow-up time increased after a testis cancer diagnosis, the standardized mortality ratios (SMR) increased, reaching a maximum of 1.64 (95% CI 1.31-2.06). after ≥30 years of follow-up.
Additionally, non-testis cancer mortality was highest among patients who were youngest at the age of testis cancer diagnosis: SMR 2.27, 95% CI 1.32-2.90 among those younger than 20 years at diagnosis.

The authors then assessed specific causes of death, the most important of which was a non-testis cancer secondary malignancy (SMR 1.53, 95% CI 1.35-1.73). As with the overall risk of mortality, SMR for non-testis cancer mortality were particularly elevated after platinum-based chemotherapy (SMR 1.43, 95% CI 1.12-1.83) and radiotherapy (SMR 1.59, 95% CI 1.34-1.89).
In particular, platinum-based chemotherapy was associated with increased risks of death from cancers of the oral cavity/pharynx, esophagus, lung, bladder, and leukemia. In contrast, radiotherapy was associated with increased rates of death from cancers of the oral cavity/pharynx, stomach, liver, pancreas, and bladder. Additionally, non-cancer mortality was also increased by both overall among testis cancer survivors (SMR 1.15, 95% CI 1.04-1.27), and specifically after platinum-based chemotherapy (1.23, 95% CI 1.03-1.47) and radiotherapy (SMR 1.17, 95% CI 1.01-1.34).
Of particular importance and interest, there was an excess of suicides following platinum-based chemotherapy (SMR 1.65, 95% CI 1.01-2.69). However, unlike some previous reports, there was no apparent significant increase in long-term overall cardiovascular mortality (SMR 1.18, 95% CI0.87-1.60). Radiotherapy was associated with an increased risk of death from digestive diseases (SMR 2.46, 95% CI 1.59-3.82).
Finally, when compared with surgery, the overall non-testis cancer mortality was increased with an increasing number of chemotherapy cycles, becoming significant after both four (HR 1.41, 95% CI 1.01-1.99) and more than four (HR 2.04, 95% CI 1.25-3.35) cycles of platinum-based chemotherapy, after >10 years of follow-up.

The authors conclude that the use of platinum-based chemotherapy and radiotherapy in the treatment of testis cancer is associated with significantly increased long-term non-testis cancer mortality, with non-testis cancer second cancers representing the most important cause of death. This effect is greatest among the youngest testis cancer patients and increases with increasing duration of follow-up. Increased risks of suicide warrant intervention to address the mental health needs of testis cancer survivors.
Presented By: Ragnhild Hellesnes, MD, Department of Oncology, University Hospital of North Norway and the University of Tromso, Norway
Written By: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center Contact: @WallisCJD on Twitter at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Virtual Annual Meeting #ASCO21, June, 4-8, 2021