Prior work from Indiana University examining 83 patients with late relapse treated between 1993-2000 suggested that surgical resection was associated with high rates of complete response and recommended that, particularly among those who previously received chemotherapy, surgical management should be the primary treatment approach.
In the Prostate, Testicular, and Penile Oral Abstract Session at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Dr. Noah Richardson presented updated data regarding the identification and treatment of patients with late relapse of germ cell tumors.
To do so, the authors drew upon the prospectively maintained Indiana University testicular cancer database. They identified 2712 pts with GCT who were treated at Indiana University between January 2000 and January 2019. The authors identified the method of detection of late recurrence, along with the treatment received, whether late recurrence was preceded by chemotherapy or not, and the survival outcomes following late recurrence. They sought, primarily, to compare progression-free survival and overall survival for patients with late relapse who were chemotherapy-naïve vs previously chemotherapy exposed. Secondarily, they considered the effect of histology (seminoma vs non-seminoma) within both the chemotherapy-naïve and chemotherapy-exposed groups.
Among the 2712 patients in the Indiana University testicular cancer database, the authors identified 90 patients with late relapse.
At the time of relapse, the median age of diagnosis was 35.2 years (range, 19.2-56.8). In terms of primary disease characteristics, 88 patients (98%) had testis primary, 1 (1%) had a retroperitoneal primary, and 1 (1%) had a mediastinal primary. The initial tumor histology was pure seminoma in 29 patients and non-seminoma in 61. At the time of relapse, 42 patients (47%) had previously received chemotherapy while 48 (53%) were chemotherapy-naïve. As we may expect, patients who previously received chemotherapy prior to late relapse had more advanced disease at the time of diagnosis (stage III, 50% vs 2%).
Interestingly, the time to late recurrence appeared to differ on the basis of both tumor histology and receipt of prior chemotherapy. Patients with non-seminoma who previously received chemotherapy had the longest time to diagnosis of late recurrence at 6.48 years median (2.02-17.0 years) while those with seminoma who had previously received chemotherapy had the shortest time (2.85 years, 2.-3.7 years).
Patterns of identification of late recurrence differed between those who had prior chemotherapy exposure as compared to those who were chemotherapy-naïve: the majority of those with prior chemotherapy exposure were detected on the basis of elevated AFP (62%) while the majority of those who were chemotherapy-naïve were identified based on routine imaging (50%).

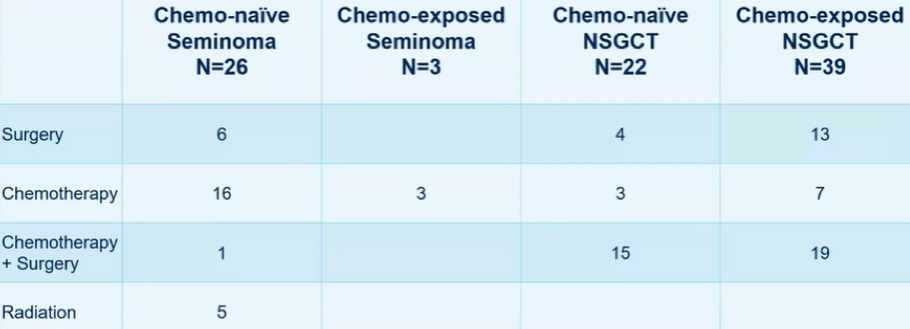
The authors then assessed treatment administered at the time of late relapse. Treatments were allocated across a variety of surgery alone, chemotherapy alone, surgery and chemotherapy, and radiotherapy, with differential use according to initial histology and prior use of chemotherapy.
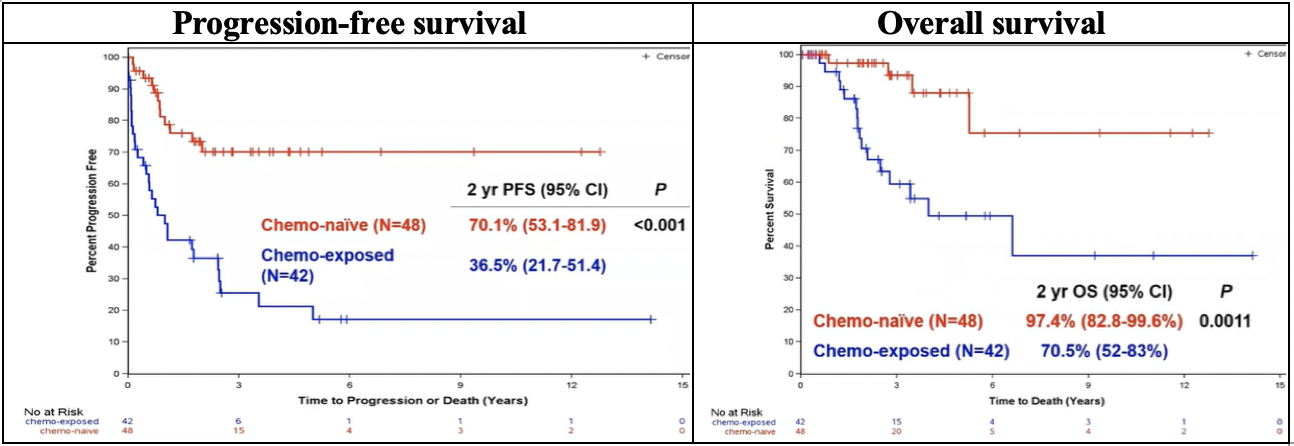
Assessing their primary outcome, the authors demonstrated significantly higher progression-free survival and overall survival for patients with late relapse who had not previously received chemotherapy.
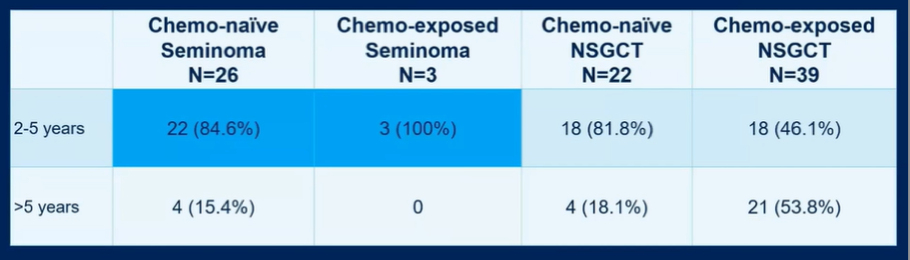
The authors then assessed this same question with somewhat more granularity, considering primary tumor histology as well. Here, they demonstrated that for progression-free survival, there was a meaningful differential effect of prior chemotherapy exposure. However, for overall survival, tumor histology appeared to be more important with patients diagnosed with seminoma having 100% two-year overall survival.

In terms of post-treatment outcomes, the authors examined outcomes of the basis prior to chemotherapy exposure. Among patients with late relapse following chemotherapy (n=42), two-year progression-free survival was 48% following surgical treatment, 10% following chemotherapy alone, and 45% following surgery and additional chemotherapy, though these differences were not significant (p=0.11) and likely reflects an underlying selection bias. Among those with late relapse in those who are chemotherapy-naïve (n=48), two-year progression-free survival was 100% following surgical resection, 74% after chemotherapy alone, and 37% following surgery and chemotherapy, differences which were significant (p=0.004) though again likely reflecting selection biases.
The authors identified next-generation sequencing results for nine patients though none had actionable findings and tumor mutational burden was low in all patients.
The authors conclude that most patients with late relapse following chemotherapy will be diagnosed as a result of elevated AFP. They further emphasized that patients with GCT require lifetime follow-up including physical examination and tumor markers. Surgical resection, when feasible, remains their preferred treatment for patients with late relapse following prior chemotherapy as chemotherapy alone offers only brief responses. However, those with chemotherapy-naïve late relapses are more likely to respond to chemotherapy at relapse.
Presented by: Noah H. Richardson, MD, Internal Medicine, Indiana University School of Medicine, Indianapolis, IN.
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center Contact: @WallisCJD on Twitter at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Virtual Annual Meeting #ASCO21, June, 4-8, 2021