Within localized disease, Dr. Heath highlighted data published in 2020 from the National Cancer Database, which includes over 214,000 men diagnosed with high-risk prostate cancer between 2004 and 2016. This disease is typically managed with either prostatectomy or radiotherapy. Black men are less likely to undergo prostatectomy from historical data, but this gap is narrowing with time. For patients treated with prostatectomy, Black men have a 20% higher mortality than white men, whereas Asian men have a 35% lower mortality than white men. From SEER data, there is a suggestion that in low-risk prostate cancer, Black men are more likely to die than white men, though it is important to note that information on causes of death is lacking in this cohort. With regards to radiotherapy, SEER data suggests that Black and Hispanic men are less likely to receive therapy. Black men have slightly higher rates of not completing radiotherapy, but when examining treatment strategies with lower numbers of total fractions (SBRT), no disparity in completion rates between Blacks and Whites has been noted.
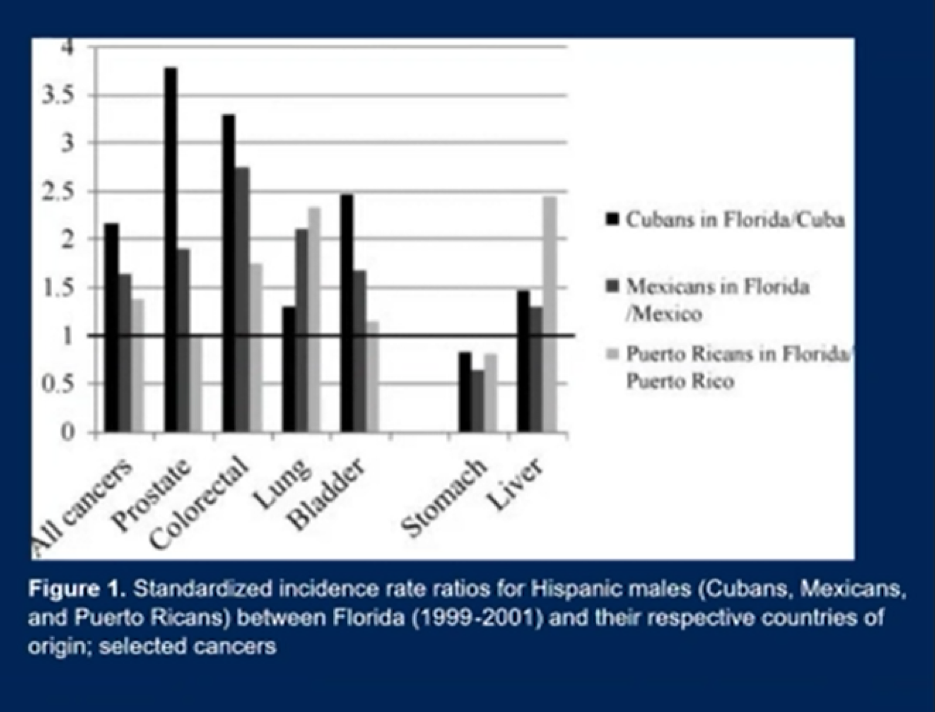
Dr. Heath also noted that ethnicity is a complex construct. For example, cancer incidence rates differ between Hispanic patients (those from Spanish-speaking countries) and Latino patients (those from Latin American countries like Brazil). She showed a figure looking at incidence rates of different cancers with Hispanic males, illustrating that the rates vary based on country of origin.
Place of residence (rural vs urban) also matters. Patients living in rural areas, even when controlling for urologist density, are less likely to receive treatment for prostate cancer. Patients in rural areas need as much supportive interventions as other patients, but data suggests the quality of life is lower for prostate cancer survivors living in rural areas. This may be due to delays in treatment resulting in more advanced disease, local cultural taboos about talking about the effects of treatment, or limited access to supportive care like mental health services. However, place of treatment (academic vs community center) research suggests that both academic and community centers have equal amounts of disparities in the treatment of minorities and uninsured patients with high-risk localized prostate cancer. This includes access to imaging studies with prostate-cancer-specific advanced imaging techniques.
Data from Switzerland suggests that patients with higher socioeconomic status have a lower risk of death than patients with low socioeconomic status. Patients with lower socioeconomic status also tended to be older at the age of diagnosis with more advanced disease/higher tumor grade.
Dr. Heath then focused on available surrounding how different racial groups respond to treatments for advanced prostate cancers. African American patients with minimally symptomatic castration-resistant prostate cancer treated with sipuleucel-T were found to have improved overall survival relative to Caucasian patients in the PROCEED registry (https://doi.org/10.1038/s41391-020-0213-7). In a meta-analysis of ten phase 3 trials of patients treated with docetaxel chemotherapy for metastatic castration-resistant prostate cancer (https:doi.org/10.1200/JCO.18.01279), researchers found equivalent median overall survival (21 months) for both Black and White men, though the pooled hazard ratio suggested a superior overall survival for Black men (HR 0.81, 95% CI 0.72-0.91). Patients treated within the Veterans Affairs system with radium-223 were found to have a decreased risk of mortality and numerically longer overall survival relative to non-Black patients (https://doi.org/ 10.1097/JU.0000000000000524). Comparisons by race for PSA responses with abiraterone acetate as front-line therapy for metastatic castration-resistant prostate cancer suggest superior median PSA progression-free survival for Black patients (16.6 months vs 11.5 months). Analysis of the 7-month PSA response rate for enzalutamide therapy as first-line treatment for metastatic castration-sensitive prostate cancer suggests equivalent rates in Black and White patients (93% vs 94%), but much lower rates for Black patients with bicalutamide (42% vs 86%). In total, these studies suggest that Black patients have equivalent or improved outcomes with therapies administered for advanced prostate cancer when administered especially in the monitored and supported setting of a clinical trial.
Finally, Dr. Heath talked about disparities in clinical trial accrual and data collection across different racial groups. She showed the following summary slide. Globally, disparities in enrollment in trial exist, with 96% of patients enrolled in the global phase 3 or 4 trials in prostate cancer identifying as White.

Efforts are underway to improve data collection and greater inclusivity in prostate cancer. One example is the IRONMAN registry, a global effort to include all men with advanced prostate cancer to provide information on care. A multilevel intervention to increase the participation of African Americans in Prostate Cancer (PAACT) initiative is also underway to help enroll African American patients into trials.
Finally, Dr. Heath provided the following suggestion slide for what providers can do to be more mindful of disparities and attempt to address them.

Presented by: Elisabeth I. Heath, MD, FACP, Hartmann Endowed Chair for Prostate Cancer Research and Professor of Oncology at the Karmanos Cancer Center, Detroit, MI
Written by: Alok Tewari, MD, Ph.D., Medical Oncologist at the Dana-Farber Cancer Institute, at the virtual 2021 American Society of Clinical Oncology Annual Meeting Congress (#ASCO21), June 4th-June 8th, 2021