The PEACE consortium (Prostate Cancer Consortium in Europe) is an academic European program that aims to conduct phase 3 trials for men with prostate cancer. This is a flexible structure that requires at least two European countries to be involved. Each trial can be sponsored by any academic hospital, and each trial is independent. Six PEACE trials have already begun accrual across various prostate cancer disease contexts.
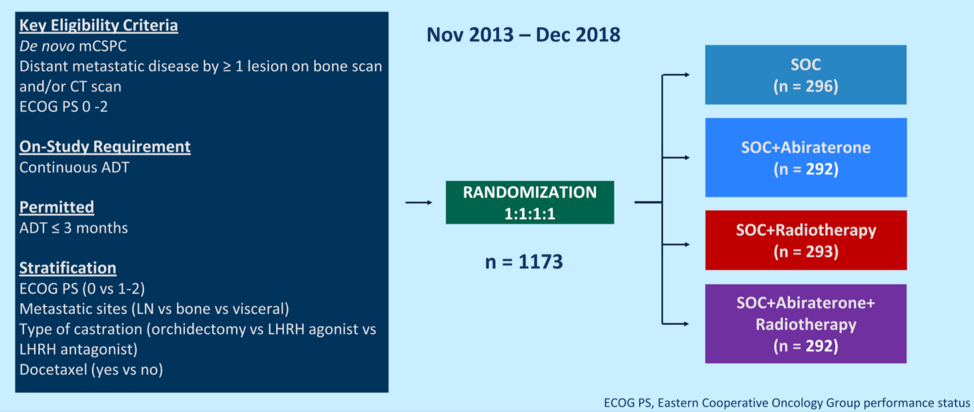
The PEACE-1 trial was sponsored by Unicancer, and 7 countries contributed to its accrual. Candidates for this trial had de novo mCSPC and could have received up to 3 months of ADT prior to randomization. Patients were stratified by metastatic site, performance status, type of testosterone lowering therapy, and the use of docetaxel. A total of 1173 men were randomized 1:1:1:1 as shown below. Standardized treatments included continuous ADT or bilateral orchiectomy, with or without docetaxel at 75 mg/m2 every three weeks for six cycles. Abiraterone treatment consisted of 1000 mg/day with prednisone 5 mg twice per day until disease progression or intolerance and was administered along with docetaxel for patients who underwent chemotherapy. Radiotherapy to the prostate was delivered in 37 doses to a cumulative dose of 74 Gy after patients completed docetaxel if receiving chemotherapy.
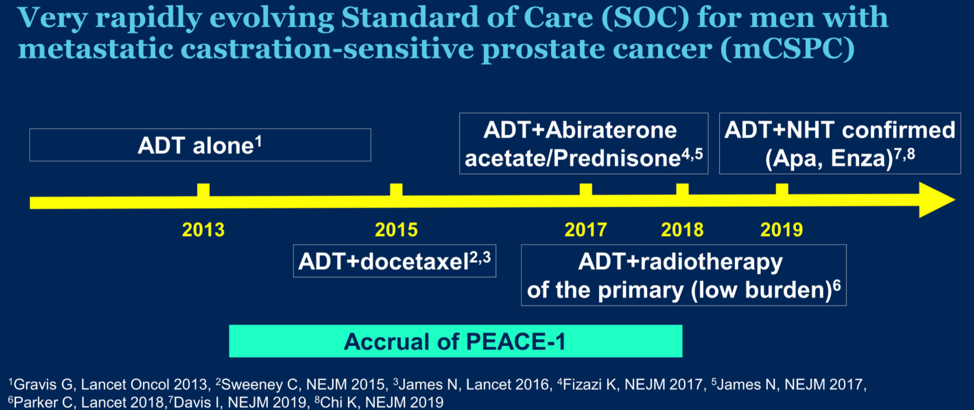
Various amendments were implemented during the course of the trial due to the evolving standard of care in this disease. After 2015, docetaxel was permitted as part of the standard of care per investigator’s discretion and patient consent. After LATITUDE and STAMPEDE were reported, it became unethical to administer ADT alone, and so docetaxel administration (without abiraterone) was made mandatory.
The two co-primary endpoints of the study were radiographic progression-free survival (rPFS) and overall survival. The trial used a 2 x 2 factorial design aimed at answering two questions, the role of abiraterone and the role of radiotherapy on top of the standard of care. To limit the risk of false-positive findings, the interaction between the effect of abiraterone and radiotherapy was tested for each endpoint. There was no evidence of interaction between abiraterone and radiotherapy in the ADT + docetaxel population, and the two abiraterone arms (with or without radiotherapy) were thus pooled for subsequent analysis. As the number of required events for the rPFS analysis for abiraterone in the ADT + docetaxel population has been reached, and therefore these results are reported here.
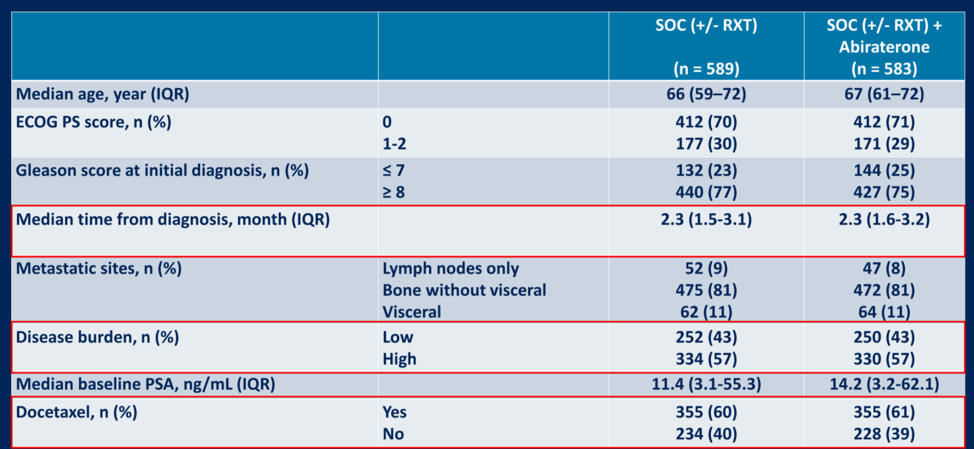
Patient characteristics are shown below randomized by abiraterone treatment. A total of 57% of patients had a high metastatic burden and 60% of patients received docetaxel.
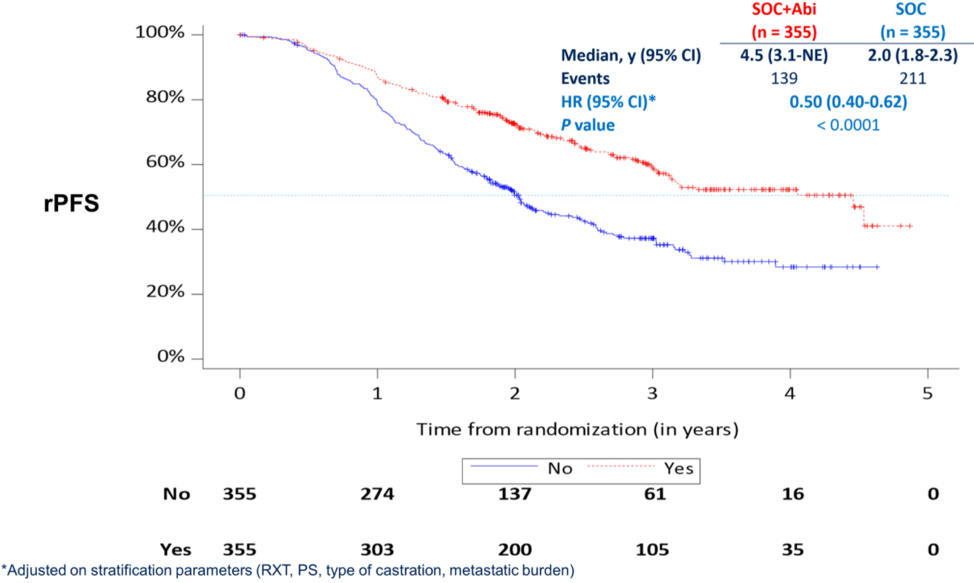
The median follow-up for the ADT + docetaxel (n = 355) and the ADT + docetaxel + abiraterone (n = 355) was 36 months. The median time to discontinuation of abiraterone in the abiraterone group was 31.4 months. The median number of docetaxel cycles administered was six.
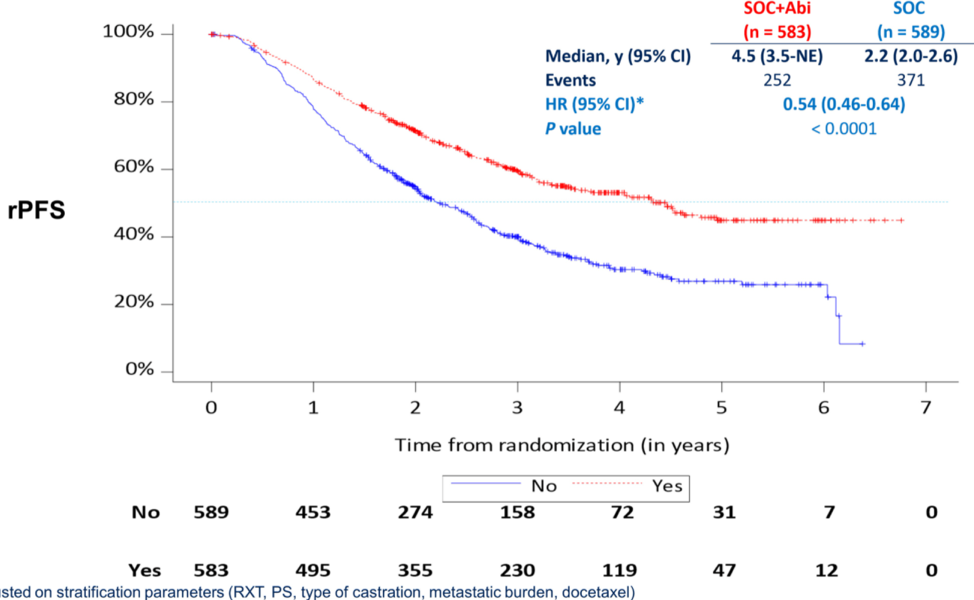
In the overall cohort, the ADT +/- docetaxel +/- radiotherapy + abiraterone arm (SOC + abi) was associated with a statistically significant improvement in rPFS relative to ADT +/- docetaxel +/- radiotherapy (SOC). Specifically, rPFS improved from a median of 2.2 years to 4.5 years, conferring a hazard ratio for progression of 0.54 (95% CI 0.46-0.64, p < 0.0001).
Per the pre-planned hierarchical testing strategy, the investigators then tested the impact of abiraterone on rPFS in patients who received ADT + docetaxel +/- radiotherapy. In this population, median rPFS was statistically significantly improved with the addition of abiraterone from 2 years to 4.5 years. Abiraterone conferred a hazard ratio for radiographic progression of 0.50 (95% CI 0.4 – 0.62, p < 0.0001).
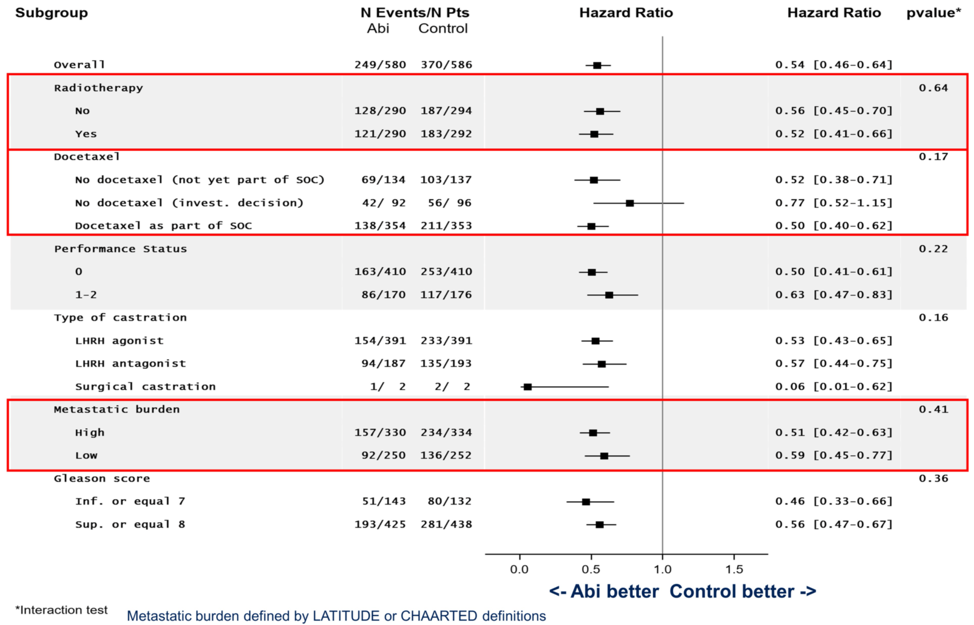
The benefit of abiraterone was consistent across subgroups analyzed.
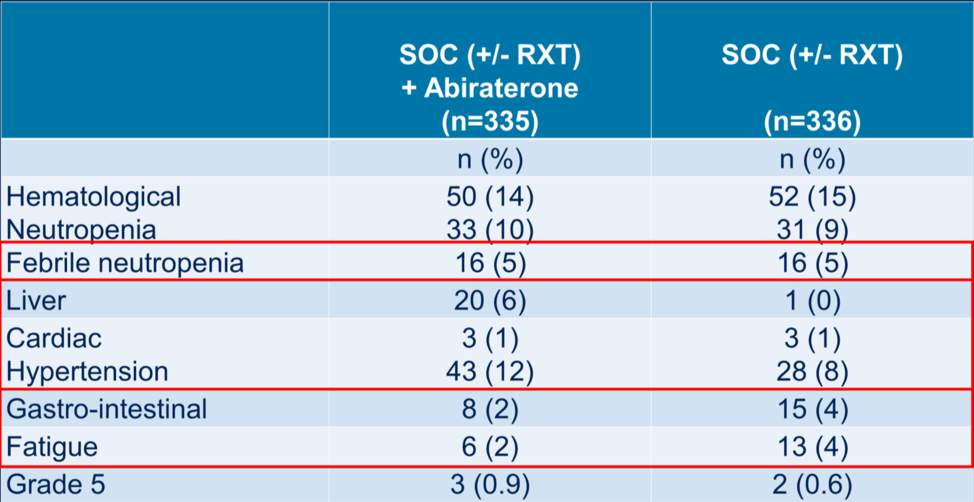
With regards to the secondary endpoint of castration-resistant prostate cancer free survival, the addition of abiraterone to both groups (ADT +/- docetaxel +/- radiotherapy and ADT + docetaxel +/- radiotherapy) conferred an absolute benefit of roughly two years and a hazard ratio for progression to CRPC of 0.40. Abiraterone also conferred a clinical progression-free benefit of approximately two years in both arms to a statistically significant degree. Within the docetaxel group, the rate of grade 3-5 toxicity was relatively similar whether abiraterone was given, with the exception of liver dysfunction and hypertension.
Dr. Karim Fizazi concluded his report of the PEACE-1 trial data by stating that the addition of abiraterone to ADT and docetaxel significantly improved radiographic progression-free survival in de novo metastatic castration sensitive prostate cancer without adding significant short-term toxicity. Overall survival data are not yet mature, so he ended by posing the question of whether triplet therapy (ADT, docetaxel, and abiraterone +/- radiotherapy to the prostate) should be incorporated as a new standard of care for patients with de novo mCSPC.
Presented by: Karim Fizazi, MD, PhD, is a medical oncologist at Gustave Roussy, and a full professor in Oncology at the University of Paris-Saclay in Villejuif, France
Written by: Alok Tewari, MD, PhD, Medical Oncologist at the Dana-Farber Cancer Institute, at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Virtual Annual Meeting #ASCO21, June, 4-8, 2021