(UroToday.com) The availability of multiple treatments for metastatic castration-resistant prostate cancer (mCRPC) mandates the need to identify, as well as validate, prognostic and predictive factors applicable to clinical practice. Given the complexity of therapeutic decision-making in these patients, there is a need to determine which patients would be most likely to benefit from a given treatment more rapidly and facilitate optimized decisions on therapeutic sequencing.
PSA value is widely used for the monitoring of treatment outcome in mCRPC in the clinical real-world setting. Early PSA changes are not considered in the definition of PSA progression due to the potential for spurious “flare” reactions. The early identification of mCRPC patients not benefiting from enzalutamide or abiraterone could be of paramount importance for optimal treatment delivery and cost-effectiveness. At the ASCO 2021 annual meeting, Dr. Fernando López-Campos and colleagues from Spain evaluated the significance of an early PSA increase in mCRPC patients treated with enzalutamide or abiraterone.
The authors retrospectively evaluated enzalutamide or abiraterone-treated mCRPC patients from 11 hospitals between 2011-2020. Early PSA progression was defined as a 25% increase in PSA from baseline at 4 or 8 weeks after treatment initiation. PSA progression at 12 weeks was confirmed by a second reading. Univariable- and multivariable Cox regression models were conducted to explore the association of PSA progression and overall survival (OS) in chemotherapy naïve patients treated with abiraterone or enzalutamide. Interaction tests were conducted to explore differences in the impact of PSA progression on OS in abiraterone or enzalutamide-treated patients.
This study analyzed 511 chemotherapy-naïve mCRPC patients treated with abiraterone (n = 391; 76.5%) or enzalutamide (n = 120; 23.5%), with a median follow-up of 30.2 months. The median duration of treatment was 14.3 months (enzalutamide: 13.7 months, 95% CI 11.0-19.5; abiraterone: 15.0 months, 95% CI 12.7-16.8). OS was longer in enzalutamide-treated patients (38.1 vs 29 months; HR 1.39, 95% CI 1.04-1.85). 59 (15.1%), 70 (17.9%) and 48 (12.3%) of abiraterone-treated and 9 (7.5%), 11 (9.2%) and 10 (8.3%) of enzalutamide-treated patients experienced PSA progression at 4 weeks, PSA progression at 8 weeks, and PSA progression at 12 weeks, respectively, although differences were not statistically significant. PSA progression was associated with worse OS at all three time points only in abiraterone-treated patients. In enzalutamide-treated patients, PSA progression at 4 weeks had a large impact on OS, not observed in PSA progression at 8 weeks or PSA progression at 12 weeks: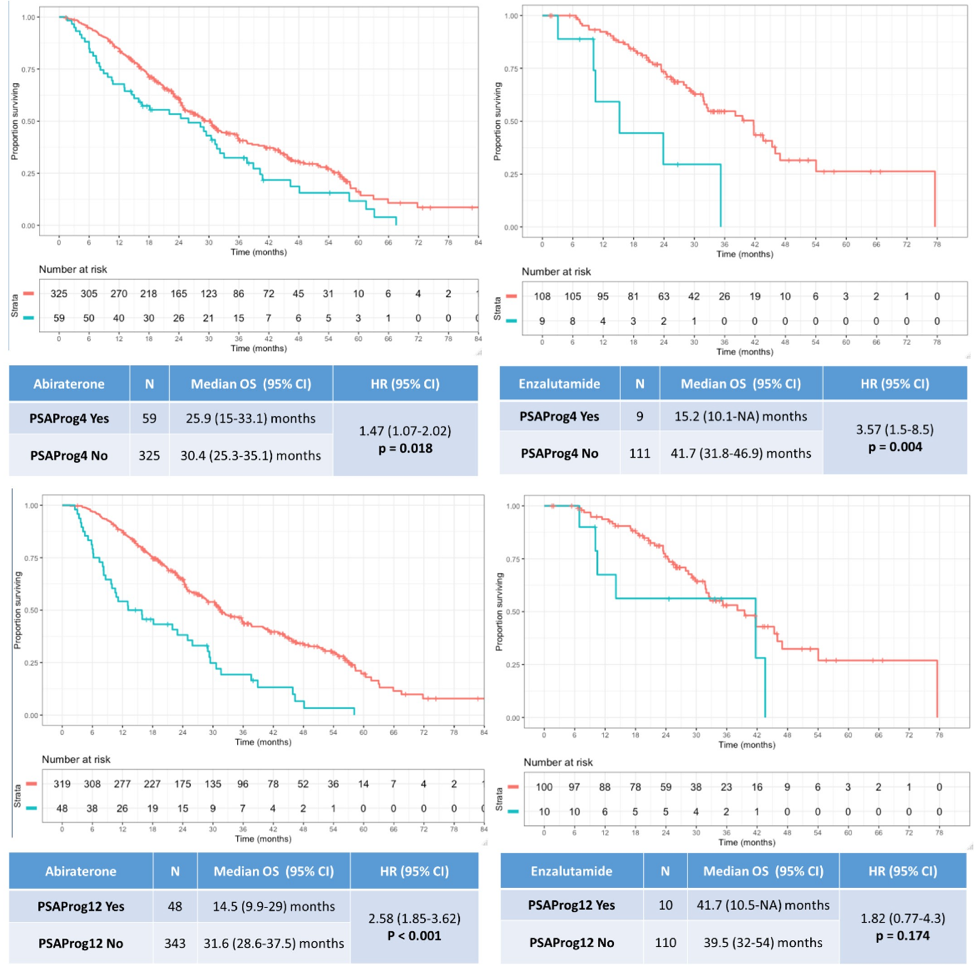
There was no significant interaction between agent (enzalutamide/abiraterone) and PSA progression.
Dr. Lopez-Campos concluded his presentation with the following summary points:
- PSA progression at 4 weeks after enzalutamide or abiraterone is significantly associated with shorter OS and may help identify patients not benefitting from enzalutamide or abiraterone before clinical or radiographic progression
- PSA pattern progression and its association with OS might differ depending on the drug used (enzalutamide or abiraterone)
- Prospective validation studies are needed to confirm these findings and establish the value of PSA progression as an early biomarker of OS in mCRPC
Presented by: Fernando López-Campos, MD, Radiation Oncology Department, Hospital Universitario Ramón y Cajal, Madrid, Spain
Co-Author: David Lorente, Casilda Llacer Perez, Miguel Ramirez-Backhaus, Paula Peleteiro, Alfonso Gomez-Iturriaga, Ivan Henriquez-López, Rebeca Lozano, Nuria Romero, Teresa Alonso-Gordoa, Javier Molina-Cerrillo, Joaquin Navarro-Castellón, Ana Castaño, Lira Pelari, Antonio Hernández-Corrales, Virginia Morillo, Raquel García, Carlos Ferrer Albiach, Elena Castro, David Olmos; Radiation Oncology Department, Hospital Universitario Ramón y Cajal, Madrid, Spain; Medical Oncology Department, Hospital Provincial de Castellón, Castellón De La Plana, Spain; Hospitales Virgen de la Victoria y Regional de Málaga, Málaga, Spain; Instituto Valenciano de Oncología, Valencia, Spain; Hospital Clínico Universitario de Santiago de Compostela, Santiago de Compostela, Spain; Radiation Oncology Department, Hospital Universitario de Cruces, Baracaldo, Spain; Hospital Universitario Sant Joan, Reus, Spain, Reus, Spain; Spanish National Cancer Research Centre, Prostate Cancer Clinical Research Unit, Madrid, Spain; Medical Oncology Department, Hospital Universitario La Princesa,, Madrid, Spain; Medical Oncology Deparment, Hospital Universitario Ramón y Cajal, Madrid, Spain; Medical Oncology Department, Hospital Universitario Ramón y Cajal, Madrid, Spain; Hospital Central de la Defensa Gómez Ulla, Madrid, Spain; Radiation Oncology Department Hospital Universitario La Paz, Madrid, Spain; Radiation Oncology Department, Hospital Provincial de Castellón, Castellón, Spain; Hospital Clínico Universitario de Valencia, Valencia, Spain; Hospitales Virgen de la Victoria y Regional de Málaga, Instituto de Investigación Biomédica de Málaga, Málaga, Spain; Spanish National Cancer Research Center (CNIO), Madrid, Spain