While discussion on this case was ongoing, an audience member posed the following question: Do you think oligometastatic prostate cancer is a potentially curable disease state? Dr. Phuoc Tran noted that he thinks oligometastatic disease is potentially curable, however, much data remains to be collected to prove this belief. He also discussed the potential role of cytoreductive surgery in this case (in addition to systemic therapy). While the data is currently best for radiotherapy to the prostate, multiple trials including TRoMbone1 are prospectively evaluating the role of surgery as a local therapy to the prostate.
Case 2: 66M who underwent robotic prostatectomy and standard pelvic lymph node dissection for pT2cN0M0 Gleason 4 + 4 adenocarcinoma. Post-op PSA was detectable at 0.04 and rose to 1.0 over the next year. CT and bone scan were negative, but a sodium fluoride PET scan showed a bony metastatic lesion to the 9th right rib. The patient was treated with 3000 cGy to the rib with a short course of androgen deprivation therapy. After two years of undetectable PSA, the patient’s PSA rose to 1.6 ng/mL. A fluciclovine PET/CT was obtained, which showed a left pelvic nodal area of avidity.
This patient was initially treated with radiation therapy to the pelvis and boost to the left pelvic node area. An audience member posed the question of whether androgen deprivation therapy is essential in combination with radiation therapy for nodal relapsed disease, and for how long. Dr. Tran discussed that while he does not think adding in ADT in this context is mandatory, there certainly may be a benefit that is not completely understood in this context, extrapolating from the known benefit of the combination of radiation and hormonal therapy in high-risk localized disease. If ADT is given, Dr. Tran assesses baseline risk using the parameters typically used for localized disease, and advocates for ADT duration based on that.
Dr. Tran also discussed whether a focused, SABR like approach is indicated for cases like this, or if a wider nodal irradiation field is preferred. He specifically described data pulled together by Piet Ost and colleagues2 comparing elective nodal therapy with stereotactic body radiotherapy. This retrospective look, likely confounded by varying rates of ADT, identified fewer nodal recurrences but higher long-term toxicity with the elective nodal approach. A clinical trial (PEACE V/STORM) is currently in process looking prospective at whole pelvic radiotherapy versus metastasis focused therapy, both in combination with ADT, for oligometastatic nodal prostate cancer metastases
Finally, Dr. Tran discussed different patterns of oligometastatic disease. Some patients who develop oligometastases will have long-term disease-free survival after metastasis-directed therapy, and could potentially be cured. Others will have metastasis-directed therapy then recur in an adjacent location – termed oligoprogressive. Most commonly, patients who oligo-progress seem to progress in the same tissue context (oligometastatic bony disease recurs in another bony site, or oligometastatic nodal disease recurs in another nodal site – though 1/3 of recurrences occur in bone in this context). The third identified category is patients from whom oligometastatic progression is just the tip of the iceberg and they eventually develop more diffuse metastatic disease.
Case 3: 66M with cT2cN1M0 Gleason 5+4 in 12/12 biopsy cores, PSA 14 ng/mL who was initially treated with radiotherapy and long-term ADT. For two years after initial therapy, his PSA remained in the 0.7-1.3 ng/mL range, but then rose to 5.4 ng/mL despite testosterone level less than 20. Imaging showed new bulky > 2.5 cm left-sided para-aortic and RP nodes.
Dr. Tran treated this patient with radiotherapy alone with a boost to the positive nodes by imaging and hopefully treating any adjacent sites of disease that were not radiographically significant. The patient sustained a PSA (nadir 0.14) and radiographic response from radiation alone. He subsequently oligo-progressed and received multiple rounds of focal therapy before eventually requiring systemic therapy with anti-androgen therapies and then chemotherapy. He discussed that there is relatively limited data for metastasis-directed therapy in oligometastatic castration resistant prostate cancer and summarized some of the studies in the table below.
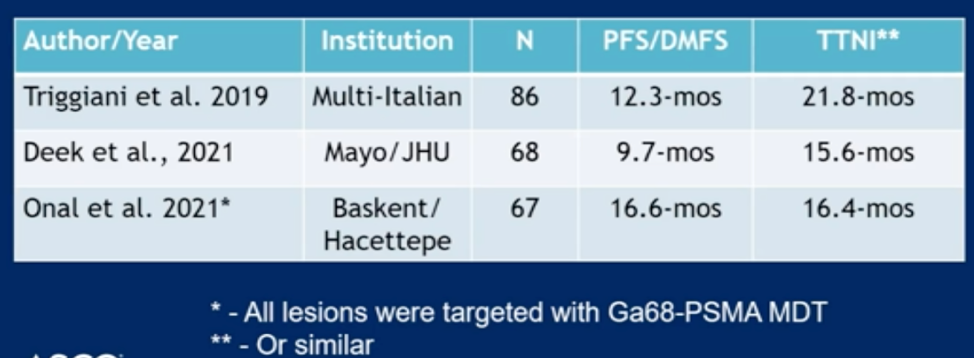
TTNI = Time to next intervention. These studies suggest that MDT does allow you to postpone treatment for at least a year but require prospective validation. The studies pending in the space are summarized below.

Dr. Tran was then asked what he means by metastasis-directed therapy. He defined it as ablative dose radiation or surgery, and SABR implies five fractions or less.
Presented by: Phuoc T. Tran, MD, PhD, Radiation oncologist at the Johns Hopkins University School of Medicine
Written by: Alok Tewari, MD, PhD, Medical Oncologist at the Dana-Farber Cancer Institute, at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Virtual Annual Meeting #ASCO21, June, 4-8, 2021
References:
- Weranja Ranasinghe, Brian F. Chapin, Isaac Yi Kim, et al. "The cytoreductive prostatectomy in metastatic prostate cancer: what the individual trials are hoping to answer." BJU International. 2020. 125, 6, 792-800.
- Elise De Bleser, Barbara Alicja Jereczek-Foss, David Pasquier et al. "Metastasis-directed Therapy in Treating Nodal Oligorecurrent Prostate Cancer: A Multi-institutional Analysis Comparing the Outcome and Toxicity of Stereotactic Body Radiotherapy and Elective Nodal Radiotherapy." European Urology. 2019. 76, 6, 732-739.