The CADMUS trial recruited 370 patients from seven sites to a prospective, multicentre, paired-cohort trial (ISRCTN 38541912). All patients underwent both mpUSS and mpMRI independently with reporting performed blinded to the result of the other study. Both radiographic studies were interpreted prior to biopsy. For both studies, a positive test defined as a Likert score of >3. Patients with either a positive mpUSS or mpMRI, or both, were advised to undergo targeted biopsies. However, they were blinded as to which test was positive. The order of mpUSS and mpMRI targeting was randomized.
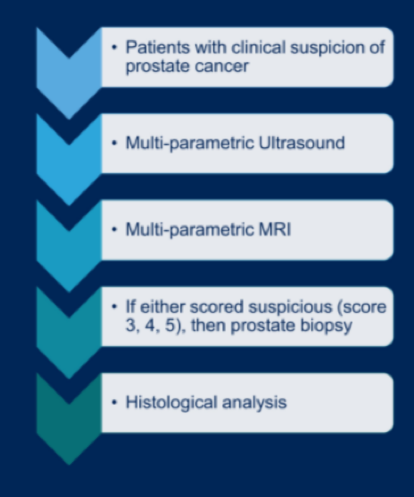
The authors assessed the primary outcomes of (1) the proportion of positive tests and (2) detection of clinically significant cancer (csPCa) defined as Gleason >4+3 of any length and/or maximum cancer core length of >6mm of any grade [PROMIS definition1].
In total, 306 patients completed both mpUSS and mpMRI. The agreement in lesion detection between the two imaging modalities was 73.2% (kappa 0.06, p = 0.14).

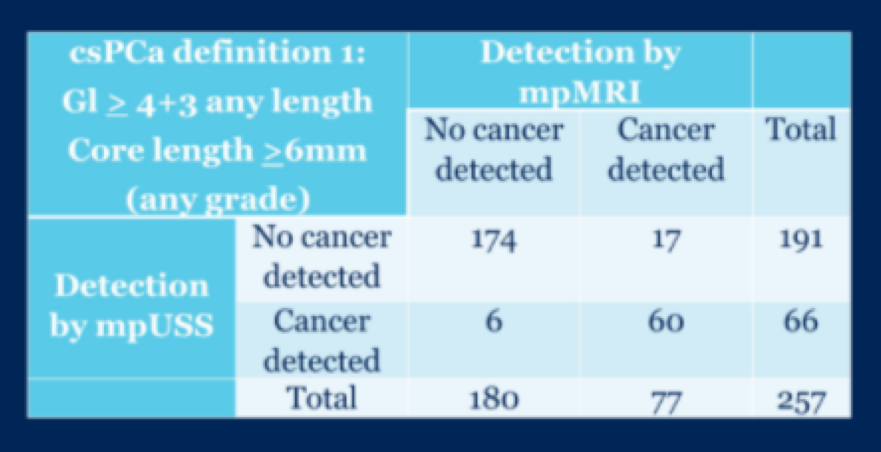
257 patients had positive results on mpUSS, mpMRI or both and, as a result, underwent targeted biopsies. Agreement between mpUSS and mpMRI for the detection of csPCa was 91.1% (expected 59.8%, kappa 0.78, p < 0.01). Overall, mpUSS detected 4.3% fewer patients with csPCa than mpMRI (95% CI = [-8.3%, -1.5%]; p = 0.042 [Bonferroni correction]). mpUSS detected 7.2% (6/83) csPCa missed by mpMRI while mpMRI detected 20.5% (17/83) csPCa that mpUSS missed.
Using a less stringent definition of significant cancer (Gleason grade >3+4 of any length), an agreement between imaging modalities was 89.1% (expected 55.6%, kappa 0.75, p < 0.01). In this case, mpUSS detected 5.4% fewer significant cancers than mpMRI overall. More specifically, mpUSS detected 7% (7/99) significant cancers according to this definition that mpMRI missed while mpMRI detected 21% (21/99) that mpUSS missed.

The authors conclude that this CADMUS trial demonstrated that mpUSS has a diagnostic performance approaching that of mpMRI. Further, the combination of both approaches increases the detection of clinically significant cancer over mpMRI alone. Additionally, mpUSS is much cheaper than mpMRI, is applicable in more healthcare settings, and is a viable approach in clinical settings in which patients cannot undergo MRI.
Presented by: Alistair Grey, Division of Surgery and Interventional Sciences, University College London, United Kingdom
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center, Contact: @WallisCJD on Twitter at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Virtual Annual Meeting #ASCO21, June, 4-8, 2021