Dr. Huang notes that the road to precision health in metastatic prostate cancer includes delivering the right therapy to the right patient at the right time. However, there are several ongoing questions that need to be addressed:
- What are the current targetable alterations in metastatic disease?
- What are the methods for testing?
- Which populations benefit from certain therapies and which do not?
Currently, there are several tests available for assessing tumor DNA mutations. Tissue or “liquid” biopsies (ie. circulating tumor cells or ctDNA) are available for multiple gene testing, including Foundation One and Tempus (both tissue-based), and EPIC, RareCyte, Guardant360, and Foundation (blood-based tests). Different tissue sources are available for obtaining samples, including bone, lymph node, liver, and soft tissue, with yields ranging from 30-75%. Currently, there is no standardized reporting of somatic mutations, but with recommendations for evaluating tumors for alterations in homologous recombination DNA repair genes, such as BRCA1, BRCA2, ATM, PALB2, FANCA, RAD51D, CHEK2, and CDK12 in patients with metastatic disease.
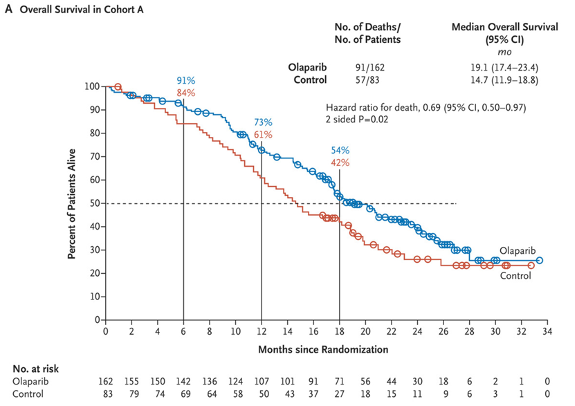
Dr. Huang highlighted that the precision oncology era for prostate cancer now includes PARP inhibitors for DNA repair mutant prostate cancer. In 2020, two PARP inhibitors were approved for use in mCRPC patients with DNA alterations, including olaparib for homologous recombination-directed repair deficiency, and rucaparib for BRCA1 or BRCA2 mutations. The PROfound study recruited men with mCRPC who had progressed on previous abiraterone acetate or enzalutamide administered at the time of non-metastatic castrate-resistant prostate cancer or at the time of metastatic castrate-sensitive prostate cancer1. Alterations were identified in one of 15 pre-specified genes involved in homologous recombination repair (BRCA 1/2, ATM, BRIP1, BARD1, CDK12, CHEK 1/2, FANCL, PALB2, PPP2R2A, RAD51B, RAD51C, RAD51D, RAD54L). Cohort A had alterations in BRCA1, BRCA2, or ATM while Cohort B had alterations in any of the other 15 included genes. In both cohorts, patients were randomized 2:1 to olaparib vs. abiraterone or enzalutamide. The primary analysis was based on imaging-based progression-free survival among patients in Cohort A. In the assessment of the primary outcome, there was a significantly improved progression-free survival in patients with mutations of BRCA1, BRCA2, or ATM (HR 0.34, 95% CI 0.25 to 0.47). Similar results were seen in the combined cohort (HR 0.49, 95% CI 0.38 to 0.63). In an updated analysis for overall survival2, the median OS for olaparib was 19.1 months versus 14.7 months in the control arm (HR 0.69, 95% CI 0.50-0.97).
Based on the results of the PROfound trial, the FDA granted approval for olaparib for deleterious or suspected deleterious germline or somatic homologous recombination repair gene-mutated mCRPC that progressed with abiraterone or enzalutamide.
The TRITON2 trial assessed rucaparib 600 mg BID in patients with mCRPC associated homologous recombination repair gene alterations3. For 115 patients with BRCA1/2 alteration, there was a 44% confirmed overall response, while patients harboring an ATM and CDK12 alteration did not receive significant benefit.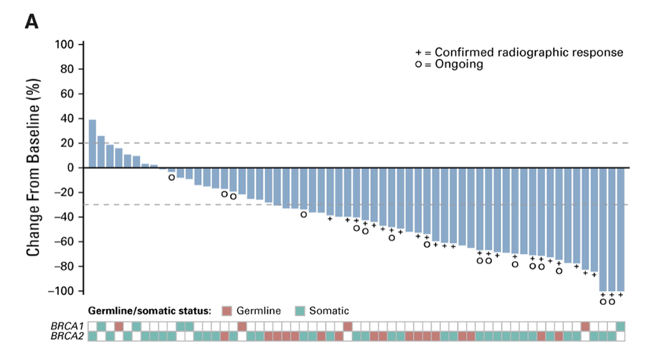
The median rPFS among 115 BRCA carriers was 9.0 months (95% CI 8.3-13.5). Based on this data, the FDA granted accelerated approval to rucaparib for men with BRCA-mutated metastatic CRPC (germline or somatic) who had prior treatment with androgen-receptor-directed therapy and prior taxane-based chemotherapy. Taken together, these data indicate the importance of genomic (somatic and germline) testing of men with mCRPC to identify mutations in genes in the DNA repair pathway who may potentially benefit from treatment with PARP inhibitors. Overall, 20-30% of mCRPC patients harbor alterations in DNA repair genes, but not all mutations benefit equally from PARP inhibition in that BRCA2, BRCA1 may be the most sensitive, whereas ATM is less sensitive.
With regards to targeting microsatellite instability-high (MSI-H) or MMRd prostate cancer, the anti-PD1 antibody pembrolizumab is FDA-approved for these tumors. However, the prevalence of MSI-H or MMRd tumors in prostate cancer is only 3.1%; tumor testing for MSI-H or dMMR using next-generation sequencing or immunohistochemistry is recommended for patients with mCRPC.
Dr. Huang notes that there are several challenges to delivering precision medicine for metastatic prostate cancer, including (i) delivering precision medicine equitably, (ii) getting tissue/genomics from difficult to biopsy tissues, (iii) using the primary biopsy vs prostatectomy specimen, (iv) obtaining metastatic biopsies (ie. lymph node, bone), and (v) and circulating tumor DNA. Specific to circulating tumor DNA, hematopoietic DNA makes up most of the cell-free DNA compartment. Normal hematopoietic cells accumulate somatic mutations during aging, which can drive clonal expansions of hematopoietic cells in the absence of dysplasia. Additional concerns regarding precision medicine include ensuring equity in treatment, given that efforts are needed to ensure that we leave no metastatic prostate cancer patients behind. Furthermore, we must ensure genomic testing and access to clinical trials amongst the most vulnerable and highest-risk populations.
Dr. Huang concluded his presentation with the following take-home messages:
- Precision medicine approaches have benefits for patients with metastatic prostate cancer
- Germline and somatic genomic testing is recommended
- Targeting MSI-high, tumor mutation burden high, and DNA repair mutations is paramount
- We must ensure equity in precision cancer medicine
Written By: Zachary Klaassen, MD, MSc, Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, June 4-8, 2021
References:
- de Bono J, Mateo J, Fizazi K, et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med 2020 May 28;382(22):2091-2102.
- Hussain M, Mateo J, Fizazi K, et al. Survival with Olaparib in Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2020 Dec 10;383(24):2345-2357.
- Abida W, Patnaik A, Campbell D, et al. Rucaparib in Men with Metastatic Castration-Resistant Prostate Cancer Harboring a BRCA1 or BRCA2 Gene Alteration. J Clin Oncol 2020 Nov 10;38(32):3763-3772.