In KEYNOTE-426, treatment-naive patients with advanced clear cell RCC, KPS ≥70%, and measurable disease (RECIST v1.1) were randomly assigned 1:1 to receive pembrolizumab 200 mg IV Q3W for up to 35 doses + axitinib 5 mg orally BID or sunitinib 50 mg orally QD on a 4-wk on/2-wk off schedule until progression, intolerable toxicity, or withdrawal. Randomization was stratified by IMDC risk (favorable versus intermediate versus poor) and geographic region (North America versus Western Europe versus Rest of World). Dual primary endpoints were OS and PFS. Secondary endpoints were objective response rate, duration of response, and safety. The protocol-specified final analysis was based on a target of 404 OS events. No formal hypothesis testing was performed because all efficacy endpoints were met previously at the first interim analysis; nominal p-values are reported.
Overall, 861 patients were randomly assigned to receive pembrolizumab + axitinib (n=432) or sunitinib (n=429). Median duration of follow-up, defined as time from randomization to the database cutoff date, was 42.8 months (range: 35.6-50.6). At data cutoff, 418 patients had died: 193 (44.7%) of 432 patients in the pembrolizumab + axitinib arm versus 225 (52.4%) of 429 patients in the sunitinib arm. The disposition of study treatment is as follows:

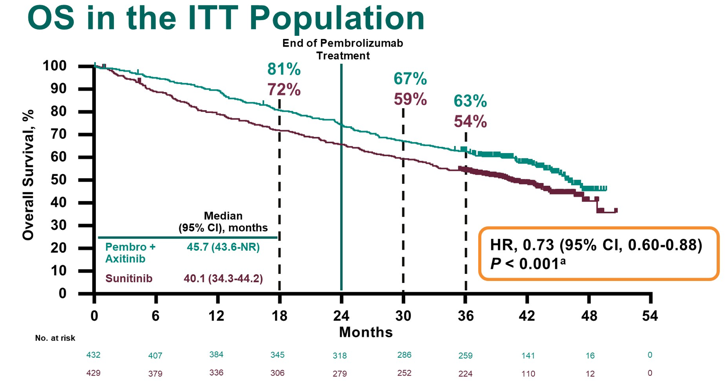
Compared with sunitinib, pembrolizumab + axitinib improved OS (median: 45.7 vs 40.1 months; HR 0.73, 95% CI 0.60-0.88)
and PFS (median 15.7 vs 11.1 months; HR 0.68, 95% CI 0.58-0.80):
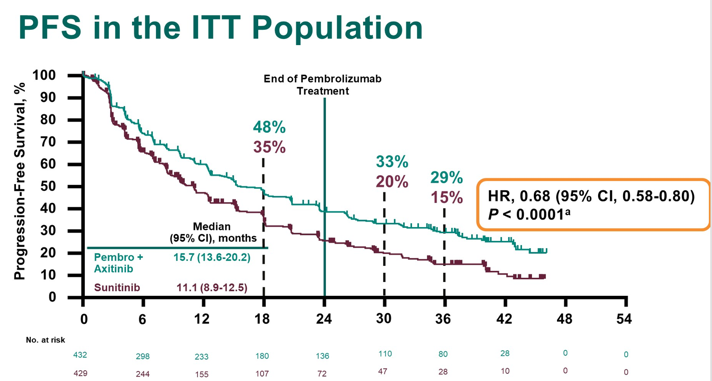
The 42-month OS rate was 57.5% with pembrolizumab + axitinib versus 48.5% with sunitinib, and the 42-month PFS rate was 25.1% with pembrolizumab + axitinib versus 10.6% with sunitinib. For pembrolizumab + axitinib versus sunitinib, the objective response was 60.4% versus 39.6% (p < 0.0001), complete response rate was 10.0% versus 3.5%
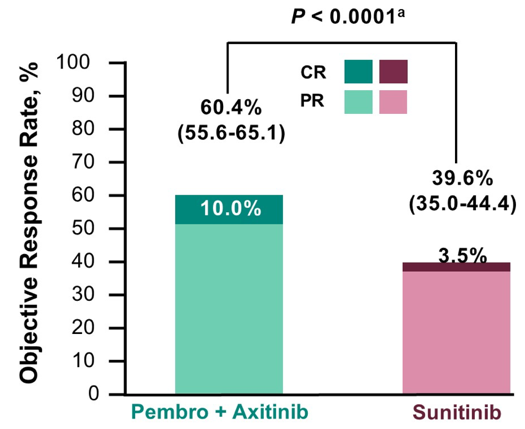
and median duration of response was 23.6 months (range: 1.4+ to 43.4+) versus 15.3 months (range: 2.3-42.8+). The efficacy results by IMDC subgroups are as follows:

Subsequent anticancer therapy was administered to 47.2% of patients in pembrolizumab + axitinib arm versus 65.5% of patients in sunitinib arm. Although a similar proportion of patients in each arm received VEGF/VEGFR inhibitors, only 10.2% of patients in the pembrolizumab + axitinib arm received subsequent treatment with a PD-1/L1 inhibitor compared to 48.7% of patients in the sunitinib arm. No new safety signals were observed. Treatment-related adverse events with incidence >= 20% within either treatment arm was most commonly diarrhea, hypertension, hypothyroidism, and fatigue:

Dr. Rini concluded this final analysis of the KEYNOTE-426 trial with the following summary statements:
- With a median follow-up of 42.8 months, KEYNOTE-426 represents the longest follow-up of an anti-PD–1/L1 immunotherapy combined with a VEGF/VEGFR inhibitor for first-line RCC.
- These results show that pembrolizumab + axitinib continues to demonstrate superior efficacy over sunitinib with respect to OS, PFS, and objective response rate, with no new safety signals
- The results of the final analysis of KEYNOTE-426 continues to support pembrolizumab + axitinib as standard of care for patients with previously untreated advanced clear cell RCC
Clinical trial information: NCT02853331
Presented by: Brian I. Rini, Vanderbilt-Ingram Cancer Center, Nashville, TN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Virtual Annual Meeting #ASCO21, June, 4-8, 2021
References:
- Rini BI, Plimack ER, Stus V, et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med 2019;380(12):1116-1127.
- Powles T, Plimack ER, Soulieres D, et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): Extended follow-up from a randomized, open-label, phase 3 trial. Lancet Oncol. 2020 Dec;21(12):1563-1573.