KEYNOTE-564 is a phase III multicenter trial of pembrolizumab versus placebo in patients with histologically confirmed ccRCC. Risk groups were defined as follows:
- Intermediate-high risk disease: pT2, grade 4 or sarcomatoid, N0 M0; or pT3, any grade, N0 M0
- High-risk disease: pT4, any grade, N0 M0; or pT any stage, any grade, N+ M0
- M1 no evidence of disease: primary tumor + soft tissue metastases completely resected ≤1 year from nephrectomy
The trial schema for KEYNOTE-564 is as follows:

Patients had undergone surgery ≤12 weeks prior to randomization, had no prior systemic therapy, and had ECOG performance status 0 or 1. Study treatment was given for up to 17 cycles (approximately 1 year). The primary endpoint was disease-free survival (DFS) per investigator assessment in all randomized patients (intention to treat population). Overall survival (OS) was a key secondary endpoint. Safety/tolerability were secondary endpoints, assessed in all treated patients.
The first prespecified interim analysis was planned after ~265 DFS events and a minimum follow-up of 12 months from the last participant enrolled. After 15 months of follow-up, 260 DFS events had occurred (78% of the planned final analysis) and 51 OS events had occurred (26% of the planned final analysis). The study had 95% power to detect a HR of 0.67 at alpha = 2.5% (one-sided) for the primary endpoint of DFS for ~990 patients. DFS was tested first at alpha = 2.5%, then alpha was passed to OS if null DFS hypothesis was rejected. The DFS and OS were estimated by the Kaplan-Meier method, and HRs and 95% confidence intervals were estimated using a stratified Cox proportional hazard model. Between-arm differences were assessed using the log-rank test.
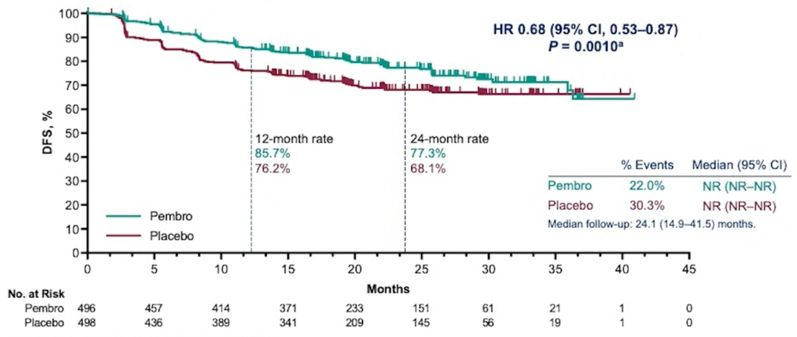
Between June 30, 2017 and September 20, 2019, 994 patients were randomized 1:1 to pembrolizumab (n=496) or placebo (n=498). As of the data cutoff date of December 14, 2020, the median follow-up, defined as time from randomization to data cutoff, was 24.1 (range: 14.9−41.5) months. No patients remain on study treatment. The participant disposition is as follows:

Baseline characteristics were generally balanced between arms. Of note, the majority of patients were M0 intermediate-high risk (86.1% in the pembrolizumab arm and 86.9% in the placebo arm). Additionally, most patients had a PD-L1 status of CPS >=1 (73.6% in the pembrolizumab arm and 76.9% in the placebo arm). At first prespecified interim analysis, the primary endpoint of DFS was met (median not reached for both arms, HR 0.68, 95% CI 0.53−0.87; p = 0.0010 [one-sided]). The estimated DFS rate at 24 months was 77.3% with pembrolizumab vs 68.1% with placebo:
Overall, DFS benefit was consistent across subgroups:

A total of 51 OS events were observed (18 in the pembrolizumab arm, 33 in the placebo arm). Median OS was not reached for both arms (HR 0.54, 95% CI 0.30−0.96; p = 0.0164 [one-sided]); the p-value did not cross the statistical hypothesis testing boundary. The estimated OS rate at 24 months was 96.6% with pembrolizumab versus 93.5% with placebo:

There were 470 patients (96.3%) and 452 patients (91.1%) experienced ≥1 all-cause adverse events with pembrolizumab versus placebo, respectively. Grade 3-5 all-cause adverse events occurred in 158 patients (32.4%) with pembrolizumab and 88 patients (17.7%) with placebo. No deaths related to pembrolizumab occurred. The most common immune-mediate adverse events were hypothyroidism (grade 1-2: 21.1% pembrolizumab arm; 3.6% placebo arm) and hyperthyroidism (grade 1-2: 11.9% pembrolizumab arm; 0.2% placebo arm).
Dr. Choueiri concluded this presentation of the KEYNOTE-564 trial with the following remarks:
- Adjuvant pembrolizumab post nephrectomy demonstrated a statistically significant and clinically meaningful improvement in DFS versus placebo in patients with intermediate-high, high risk, or M1 no evidence RCC
- Additional follow-up is planned for the key secondary endpoint of OS
- The benefit was consistent across subgroups, including the M1 no evidence of disease population, potentially extending the use of pembrolizumab to these patients
- Safety results were in line with expectations and no new safety signals were observed, with a low incidence of high-dose corticosteroid treatment for immune-mediated adverse events
- KEYNOTE-564 is the first positive phase III study with a checkpoint inhibitor in adjuvant RCC, and these results support pembrolizumab as a potential new standard of care for patients with RCC in the adjuvant setting
As a final thought, Dr. Choueiri notes that we have come a long way to find a meaningful phase 3 trial in the adjuvant RCC setting, with the first randomized controlled trial presented at ASCO in 1992 assessing the impact of interferon-alpha-2a in the adjuvant setting. Nearly 30 years later we have meaningful data for this important population of RCC patients.
Clinical trial information: NCT03142334
Presented by: Toni K. Choueiri, MD, Dana-Farber Cancer Institute, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Virtual Annual Meeting #ASCO21, June, 4-8, 2021