This study pooled data from trials submitted for FDA review of a checkpoint inhibitor combination as first-line treatment for patients with metastatic RCC. Trials were included only for those with available data for stage at initial diagnosis to identify patients with stage IV disease at initial diagnosis and to exclude those with nephrectomy in the non-metastatic setting. Kaplan-Meier method was used to estimate median OS in patients with de novo metastatic RCC with and without nephrectomy prior to immunotherapy-based combination therapies. The study schema is as follows:
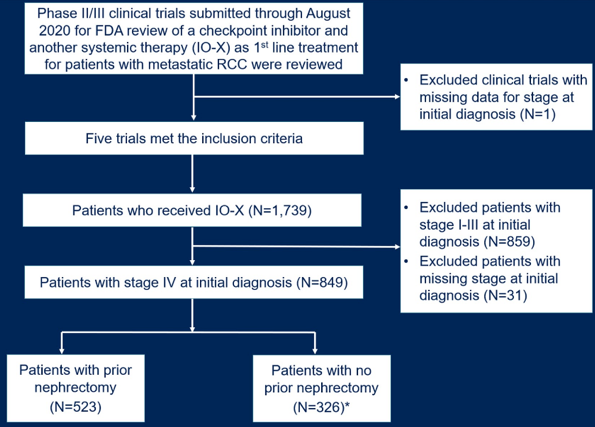
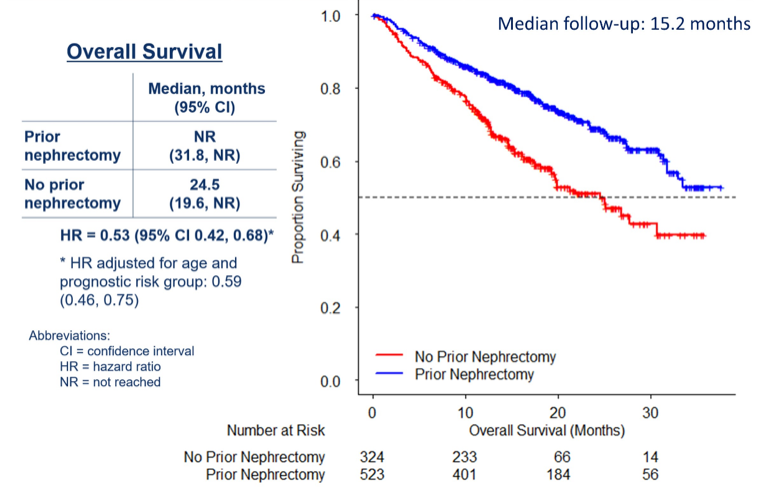
There were five trials that met inclusion criteria, all of which evaluated immunotherapy in combination with a kinase inhibitor. Data for stage at initial diagnosis was available in 1,708 patients who received immunotherapy-based combination therapies. The majority of patients were male (72%) and white (80%). Among the 849 patients (50%) with stage IV RCC at initial diagnosis, 523 patients (62%) had nephrectomy prior to immunotherapy-based combination therapies. All patients had clear cell histology and sarcomatoid differentiation was present in tumor pathology of 25% and 10% of patients with and without prior nephrectomy, respectively. The proportion of patients with favorable, intermediate, and poor-risk disease was 10%, 70%, and 20%, respectively. OS appeared better in those with stage IV disease at diagnosis who had prior nephrectomy compared to patients without nephrectomy (HR 0.53, 95% CI 0.42 to 0.68), even after adjusting for age and prognostic risk group (HR 0.59, 95% CI 0.46 to 0.75):
Dr. Fallah concluded her presentation with the following take-home messages:
- In this retrospective, exploratory analysis, nephrectomy prior to immunotherapy-based combination therapies in patients with a new diagnosis of stage IV RCC appeared to be associated with improved OS, even when controlling for age and prognostic risk group
- The decision for nephrectomy is affected by factors such as medical comorbidities which could not be completely controlled
- Results should be considered hypothesis-generating
Presented by: Jaleh Fallah, MD, U.S. Food and Drug Administration, Silver Spring, MD
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Virtual Annual Meeting #ASCO21, June, 4-8, 2021