Case: 62F presents with gross hematuria and undergoes cystoscopy.
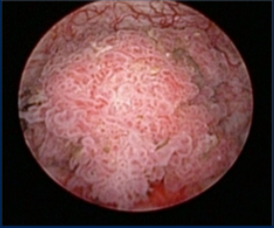

She is diagnosed with carcinoma in situ (CIS) and receives intravesicular BCG for six treatments followed by maintenance therapy. After six months of maintenance therapy, her surveillance cystoscopy reveals recurrence carcinoma and situ and a new invasive T1 urothelial carcinoma.

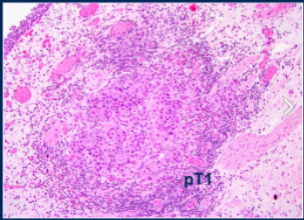
Dr. Vapiwala then commented on the pathology from the TURBT, which reveals invasion of the muscularis mucosa of the lamina propria. Muscle invasion is defined as invasion of the muscularis propria, and so to accurately assess this there needs to be muscularis propria present in your resection/biopsy specimen. This is a high-grade disease due to the presence of dense nuclei and invasion of muscularis mucosa but not muscularis propria, so we would call this pathologic T1 high-grade disease.
The first question posed was “What treatment option would you proceed with?”. (A) Intravesical chemotherapy, (B) Intravenous pembrolizumab, (C) Radical Cystectomy, or (D) Other.
Expert consensus in this discussion was that radical cystectomy is the best option for long-term disease control.
The patient is not interested in radical cystectomy or intravenous pembrolizumab due to travel requirements. She is willing to receive intravesical chemotherapy with gemcitabine and docetaxel. After intravesical chemotherapy, surveillance cystoscopy performed 6 months later reveals invasive disease obscuring the bilateral ureteral orifices, resulting in kidney injury. CT imaging reveals bilateral hydronephrosis but no significant lymphadenopathy. Bilateral percutaneous nephrostomy tubes are recommended, and the patient wants to start treatment as soon as possible. Her ECOG PS is 1 and she has no other major comorbidities. What options do you consider? (A) Radical cystectomy, (B) Split-dose cisplatin-combination chemotherapy followed by cystectomy, (C) carboplatin-combination chemotherapy followed by cystectomy, (D) pembrolizumab followed by cystectomy, (E) Bladder preservation with cisplatin-based chemoradiation, (F) Bladder preservation with 5FU based chemoradiation.
Dr. Vapiwala discussed that weighing patient wishes and goals of care in each context is really important, especially because there is an interest in bladder preservation trimodality therapy. This refers to maximal transurethral resection of bladder tumor followed by radiation and concurrent radiosensitizing chemotherapy. This has historically been chosen for patients who are deemed unfit for radical cystectomy or who refuse. Many clinical trials exclude patients with specific conditions that are typically related to poor prognosis (tumor greater than 6 cm, hydronephrosis, etc) and so these would need to be incorporated into the counseling of every patient’s specific context. The importance of multi-disciplinary discussion cannot be overstated. We also have more promising initial trial data that other chemotherapies other than cisplatin can be used for concurrent chemoradiation along with more sophisticated radiotherapy techniques. For this patient, I would want to know how her kidney function trends, and what her motivations with treatment are, and whether she might be interested in bladder preservation understanding that salvage cystectomy may be possible down the line. This would involve chemoradiation and then seeing if there is a good response, and if not, proceeding with radical cystectomy.
With bilateral nephrostomy tubes, the creatinine clearance improves to 61 ml/min and becomes cisplatin eligible. She prefers surgery but would be willing to receive neoadjuvant chemotherapy is recommended. The patient undergoes neoadjuvant dd MVAC and then radical cystectomy with an ileal conduit. Pathology reveals ypT2N0 disease. What course of action would you recommend next? (A) Adjuvant carboplatin with gemcitabine, (B) Adjuvant taxane-combination chemotherapy regimen, (C) Adjuvant checkpoint inhibitor, (D) Observation
The largest data set regarding adjuvant radiation therapy is a National Cancer Database study published in 2018. This study suggested while there was no overall survival benefit with adjuvant radiation in all patients, patients with positive surgical margins did have an overall survival benefit. One risk stratification criteria for trying to avoid locoregional recurrence is the Penn risk stratification method, which incorporates pathological T stage, margin status, and the number of lymph nodes identified during surgery. With regards to margin status, the location of the positive margin appeared to be important, with the highest risk of locoregional recurrence associated with a positive margin at the external/internal iliac region. While there are definitely toxicity concerns, intensity-modulated radiotherapy with image guidance can drastically reduce the risk to adjacent organs such as the bowel. For this patient, if a margin was positive, I would discuss the implication of the margin location, assess her overall function, and see how she felt about it as well.
The patient undergoes observation. Six months later, surveillance CT imaging reveals the following image. Creatinine clearance is now 48 ml/min and ECOG performance status is 1. Would you perform PD-L1 IHC on archival tissue to aid in treatment decision-making?

Much of the intervening discussion focused on medical oncology options for systemic therapy.
The patient responds to enfortumab vedotin for 9 months before developing increasing back pain. ECOG PS is now 3. After obtaining a spine MRI, what will be your next course of action? (A) Hospice, (B) Radiation therapy, (C) Surgical decompression, (D) Palliative chemotherapy and bisphosphonates.

Emerging data suggest that SBRT is superior for providing pain relief compared to conventional therapy and may improve clinical outcomes beyond pain control. Dr. Vapiwala would favor aggressive palliation with pain medication as well as SBRT to the lesion causing pain.
The session ended with key take-home points, which are shown below.

Presented by: Neha Vapiwala, MD, Radiation Oncologist at the University of Pennsylvania, Philadelphia, PA
Written by: Alok Tewari, MD, Ph.D., Medical Oncologist at the Dana-Farber Cancer Institute, at the virtual 2021 American Society of Clinical Oncology Annual Meeting Congress (#ASCO21), June 4th-June 8th, 2021