Data from over 20 years ago from a small series of cT2-T3N0M0 patients treated with TURBT and MVAC chemotherapy showed long-term survival in a subset of patients who elected to forgo cystectomy. Limitations to more widespread adoption of bladder-sparing treatment approaches include a lack of rigorous methods to measure and define clinical complete response and a lack of understanding of the role of salvage or delayed cystectomy for patients who experience a local recurrence. More recent molecular data suggest that combining cisplatin and immunotherapy in combination with TURBT may provide patient benefit, especially for tumors harboring DNA damage repair alterations and/or high tumor mutational burden.

To address the above limitations and further evaluate the potential role of bladder-sparing management of MIBC, Dr. Galsky and colleagues designed the HCRN GU16-257 trial in 2015, the schema of which is shown below. Clinical complete response (cCR) was defined as: (1) no abnormalities on post-cycle #4 imaging, (2) no abnormalities on post cycle #4 urine cytology, and (3) less than or equal to low-grade Ta tumor on post cycle #4 bladder biopsy. The primary endpoint was the cCR rate, and the co-primary endpoint was the ability of cCR to predict benefit, which was defined as the 2-year metastasis-free survival in patients pursuing surveillance, or pCR rate in patients who undergo cystectomy. The sample size was designed such that the lower bound of the confidence interval for the positive predictive value of cCR exceeds 80%.
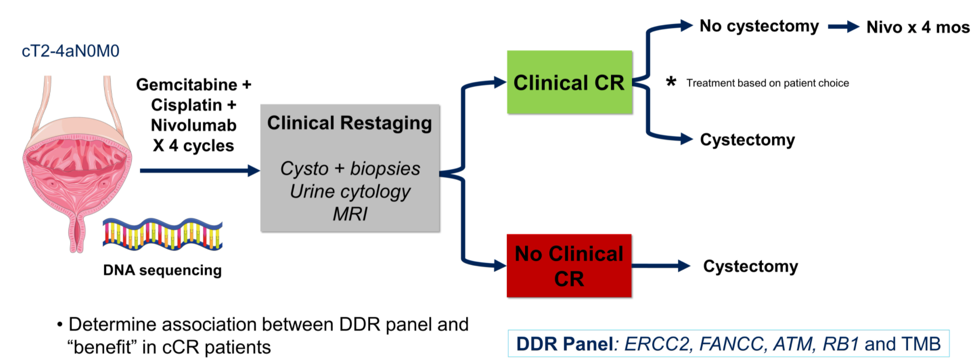
This trial was written before much of the molecular data supporting DNA damage alterations and tumor mutational burden/PD-L1 status as biomarkers for drug response became clear, and so all biomarker work from this trial is exploratory rather than used for stratification.
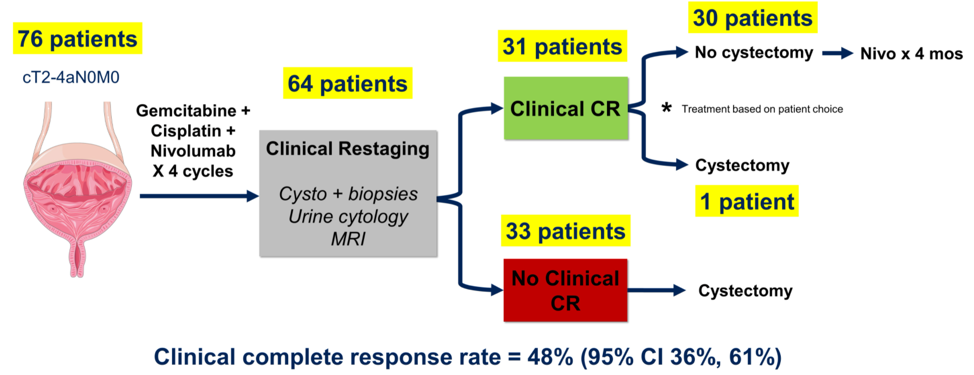
In total, 76 patients were enrolled on study. Of the enrolled patients, 79% were male, with a median age of 69. Most patients had cT2 disease (57%), 32% had cT3 disease, and the rest had cT4. 76% of patients had transitional cell carcinoma, and the rest had a variant histology.
The patient outcomes are shown below. The cCR rate was 48%. Of the 31 patients with cCR, 22 have not had any recurrence, and all patients with cCR remain alive at last follow-up. Only one patient with cCR has had evidence of metastatic disease recurrence at approximately 19 months. The rest either opted for immediate cystectomy (1 patient) or had local recurrence and underwent delayed cystectomy.
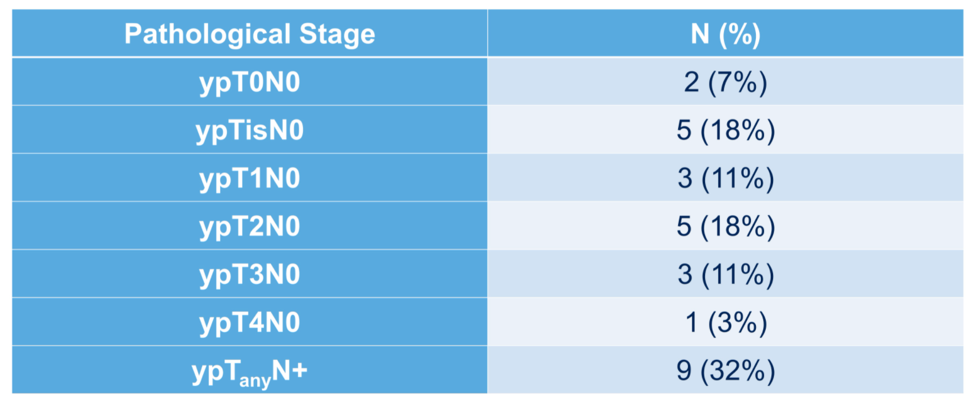
The six patients who underwent delayed cystectomy after local recurrence had pathological findings as shown below:

This is in contrast to the pathological distribution of findings in patients that did not achieve a cCR.
The adverse event profile observed was consistent with other studies of chemotherapy plus PD-1 blockade.
Exploratory genomic correlative analyses are shown below. High tumor mutational burden (> 10 Muts/Mb) and the presence of ERCC2 mutation were significantly associated with clinical response. Genomic alterations in ATM, FANCC, or RB1 were not associated with clinical response. An oncoplot of the genomic studies is shown below with clinical annotation.

Dr. Galsky concluded that TURBT and gemcitabine/cisplatin chemotherapy in combination with nivolumab is associated with cCR as defined in this trial in almost half of the patients with MIBC enrolled in this study. The durability of responses requires ongoing follow-up, and genomic as well as radiomic biomarkers are being explored as potential predictors of cCR and long-term bladder-intact recurrence-free survival.
Presented by: Matt Galsky, MD, Professor of Medicine and Director of Genitourinary Medical Oncology at the Tisch Cancer Institute, Mount Sinai Hospital, New York, New York.
Written by: Alok Tewari, MD, PhD, Medical Oncologist at the Dana-Farber Cancer Institute, at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting, Virtual Annual Meeting #ASCO21, June, 4-8, 2021