LBA1 – Maintenance avelumab + best supportive care (BSC) versus BSC alone after platinum-based first-line chemotherapy in advanced urothelial carcinoma: JAVELIN Bladder 100 phase II interim analysis
In this study, the authors demonstrated an overall survival benefit with maintenance avelumab in patients that did not progress (complete response, partial response, or stable disease) on at least four cycles of induction platinum-based chemotherapy for advanced urothelial carcinoma.
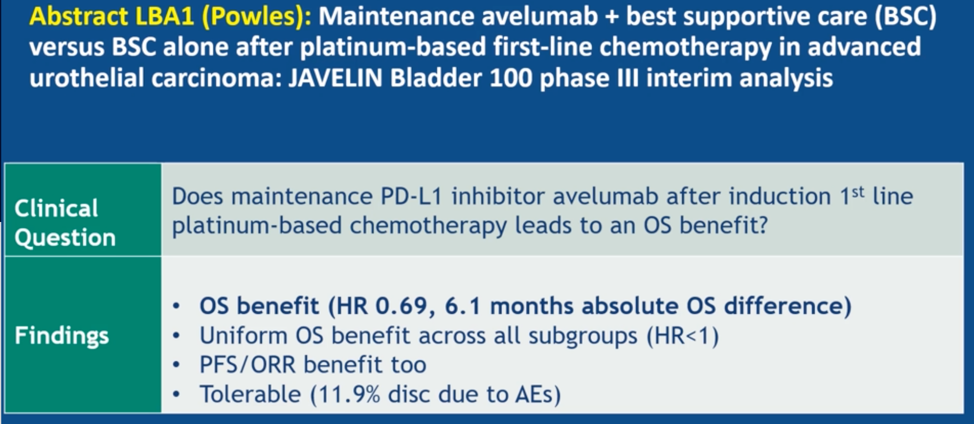
Dr. Choueiri commented that this is the first switch-maintenance immunotherapy after chemotherapy trial to read out as positive for overall survival benefit in solid tumors and is likely to be an immediate practice change for urothelial cancer treatment. One question he raised is whether a shorter duration of immunotherapy would be equally effective as treating with avelumab to progression. Dr. Choueiri also noted that patients whose tumors were negative for PD-L1 expression or had visceral metastases (poor prognosis overall) seemed to derive less benefit than other patients on trial and asked whether these patients should receive treatment intensification.
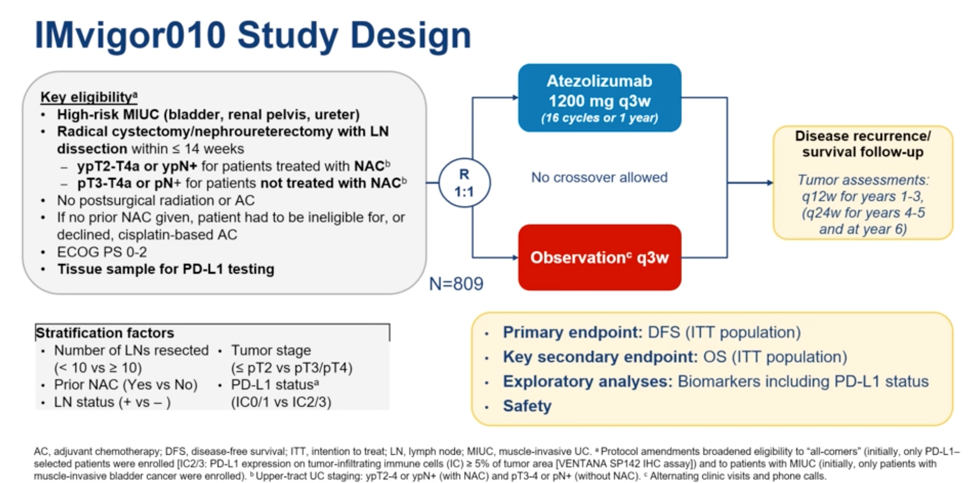
Abstract 5000 – Imvigor010: Primary Analysis from a Phase III Randomized Study of Adjuvant Atezolizumab vs Observation in High-Risk Muscle-Invasive Urothelial Carcinoma.
The standard of care for muscle-invasive urothelial carcinoma consists of neoadjuvant cisplatin-based chemotherapy if possible followed by radical cystectomy. The optimal adjuvant management of these patients is not established. Atezolizumab is approved for second-line therapy in metastatic urothelial carcinoma. In this study, the investigators tested the utility of atezolizumab as an adjuvant therapy by randomizing high-risk patients with muscle-invasive bladder cancer after cystectomy to either observation or q3w atezolizumab as adjuvant therapy for up to 16 cycles. The primary endpoint was disease-free survival in the intention-to-treat population, and the secondary endpoint was overall survival.
This study did not meet its primary endpoint of improved disease-free survival with adjuvant atezolizumab, regardless of PD-L1 expression within the tumor.
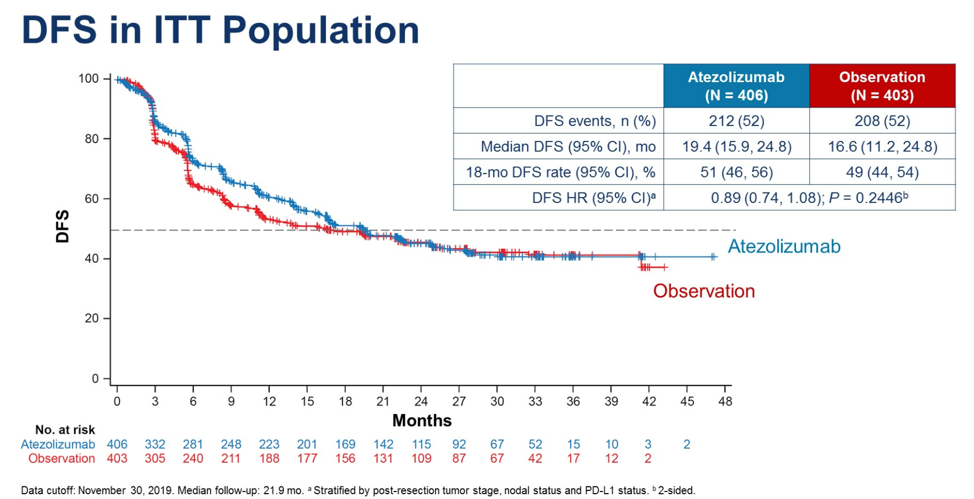
At 21.9 months of median follow-up, the median overall survival in either cohort had not been reached, and there was no significant difference in survival at the data cut-off between observation and atezolizumab.
Dr. Choueiri concluded that adjuvant PD-L1 therapy is not currently advisable in unselected patients with muscle-invasive bladder cancer after cystectomy. However, he notes that it may be possible to identify patients who would benefit from adjuvant therapy by epigenetic profiling or predict patients more likely to respond to atezolizumab using biomarkers similar to those discussed in Abstract 5011 (high PD-L1 expression plus high tumor mutational burden). Given the overall high-risk for cancer-specific mortality in patients with muscle-invasive bladder cancer, it will be important to continue to do adjuvant trials to try and improve patient outcomes.
Abstract 5001 – Pembrolizumab Plus Axitinib Versus Sunitinib as First-Line Therapy for Advanced Renal Cell Carcinoma: Updated Analysis of KEYNOTE-426
In this abstract, the authors provide 23-month progression-free and overall survival updates for patients with advanced renal cell carcinoma treated on KEYNOTE-426 with pembrolizumab and axitinib as compared to sunitinib. The initial interim analysis data published in 2019 showed improved survival and progression-free survival with combination immunotherapy and TKI therapy relative to TKI therapy with sunitinib. The trial schema is shown here:

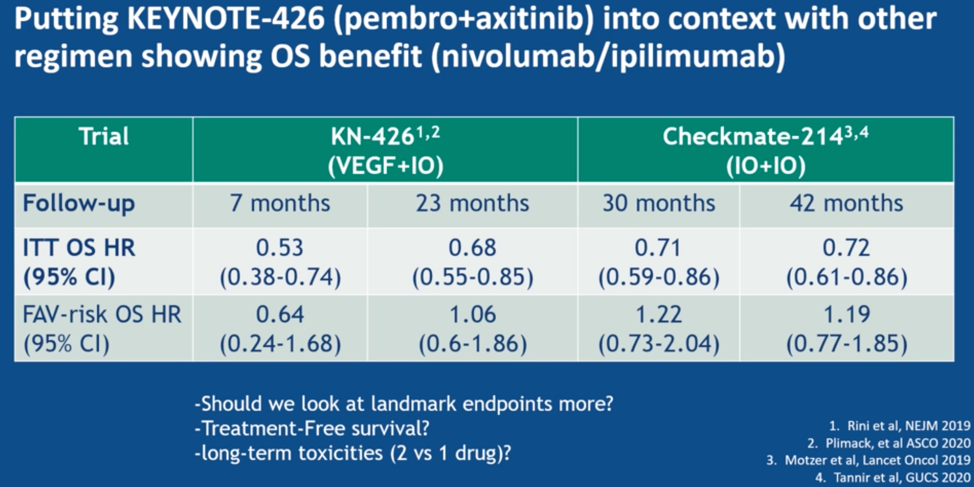
Updated outcome data were summarized as below:
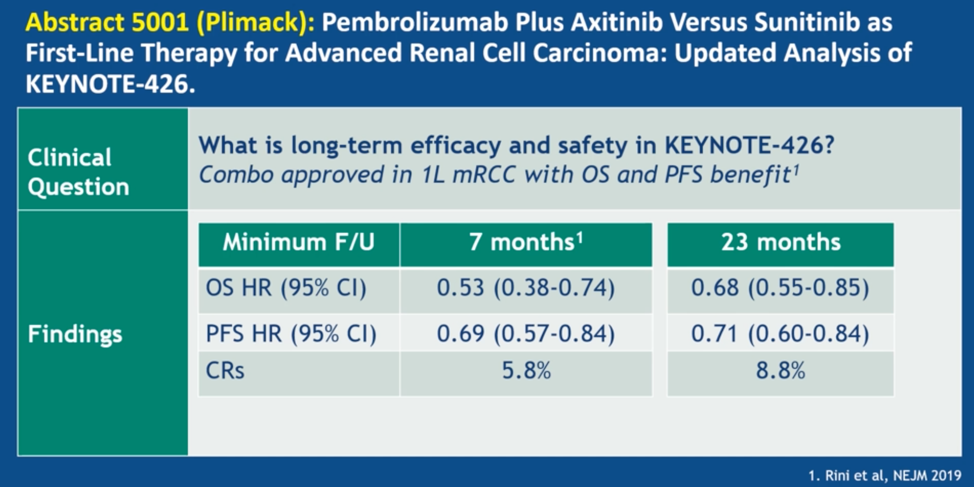
At extended follow-up, there were no new safety concerns. The relationship between pembro + axi treatment and overall survival was significant in the IMDC intermediate/poor risk groups, and numerically better in the IMDC good risk treatment group. The authors also pursued a 6-month landmark analysis to explore the relationship between the depth of response and survival. These analyses suggested that greater depth of tumor shrinkage was associated with overall survival in the pembro + axi arm.
Dr. Choueiri then put this trial in context with results from the Checkmate-214 trial of nivo/ipi, which showed an overall survival benefit in the intention-to-treat population, but non-statistically significant association with treatment and survival for the IMDC favorable risk group.
He ended with describing future directions for treatment in advanced renal cell carcinoma, showing the following slides:

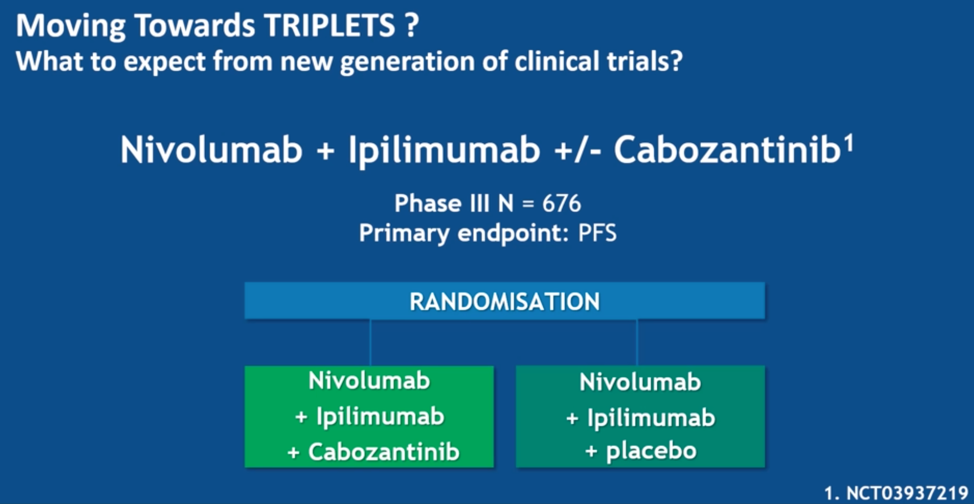
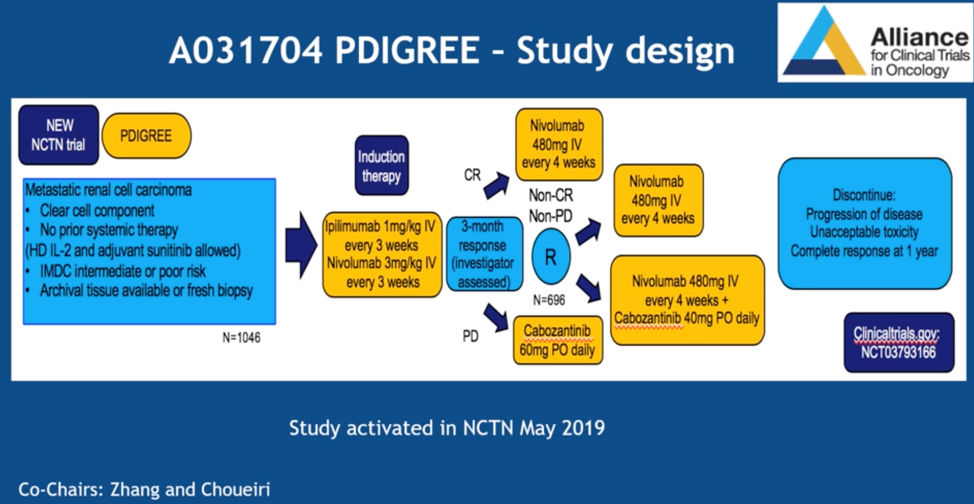

Overall, these trials are generally moving away from sunitinib as the control arm, and are investigating either triplet therapies, the addition of cabozantinib to therapeutic combinations, or novel therapeutic agents such as the HIF inhibitor MK6482.
Abstract 5006 – Phase II study of nivolumab and salvage nivolumab + ipilimumab in treatment-naïve patients (pts) with advanced renal cell carcinoma (RCC) (HCRN GU16-260).
Combination nivolumab and ipilimumab is approved for treatment naïve IMDC intermediate and poor-risk clear cell renal cell cancer (ccRCC) based on the Checkmate-214 study, and nivolumab monotherapy is approved for post-tyrosine kinase inhibitor treatment of ccRCC, This study aimed to dissect the response rate to nivolumab monotherapy in treatment naïve ccRCC, and identify the salvage response rate for nivolumab monotherapy with combination nivolumab and ipilimumab.

The data are summarized above, with a 32% overall response rate with nivolumab monotherapy in treatment naïve ccRCC, and an overall response rate of 13% with salvage nivolumab and ipilimumab. No complete responses were identified.
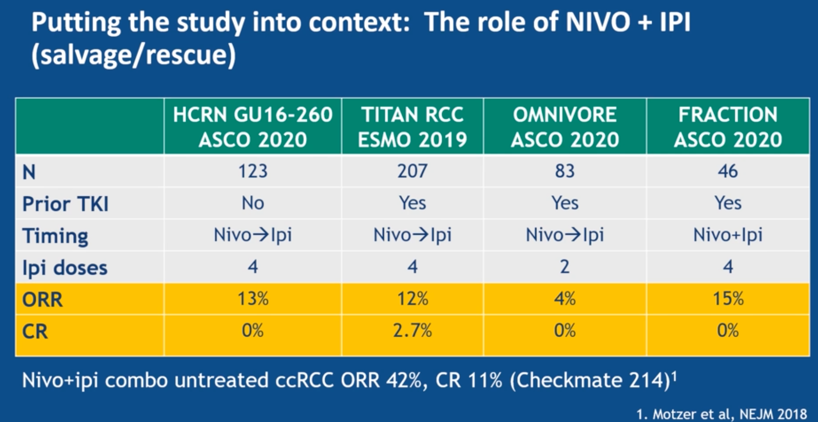
Dr. Choueiri then showed the above slide, overall comparing the overall response rates of sequential and combination therapy for nivolumab and ipilimumab. The ORRs are quite low compared to the combination therapy in untreated ccRCC from Checkmate-214. He concluded that the strategy of single-agent nivolumab followed by ipilimumab salvage cannot be recommended at this time, especially since many patients are unable to receive salvage immunotherapy.
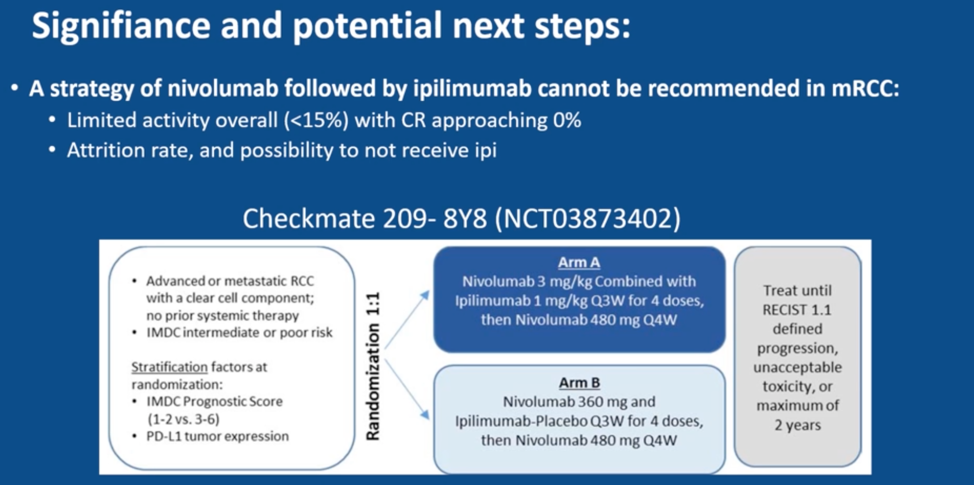
Finally, he highlighted the Checkmate 209-8Y8 trial looking at nivolumab maintenance in intermediate to poor-risk metastatic ccRCC, which may help further delineate the role of nivolumab monotherapy in this disease.
Presented by: Toni K. Choueiri, MD, Director of the Lank Center for Genitourinary Oncology and Professor of Medicine, Dana-Farber Cancer Institute and Harvard Medical School, Boston, MA
Written by: Alok Tewari, MD, Ph.D., Medical Oncology Fellow at the Dana-Farber Cancer Institute, at the 2020 American Society of Clinical Oncology virtual annual meeting (#ASCO20), May 29th-May 31st, 2020 at the 2020 ASCO Annual Meeting, Virtual Scientific Program #ASCO20, May 29-31, 2020.
Related Content:
Read: ASCO 2020: JAVELIN Bladder 100 Phase III Results: Maintenance Avelumab + Best Supportive Case vs BSC Alone After Platinum-Based First-Line Chemotherapy in Advanced Urothelial Carcinoma
Read: ASCO 2020: IMvigor010: Primary Analysis from a Phase III Randomized Study of Adjuvant Atezolizumab versus Observation in High-Risk Muscle-Invasive Urothelial Carcinoma
View: KEYNOTE-426: Pembrolizumab plus Axitinib versus Sunitinib as First-Line Therapy for Advanced Renal Cell Carcinoma (RCC) - Brian Rini