Advanced or metastatic bladder cancer (mUC) represents a particularly difficult population as treatment options are rarely curative and patient outcomes are quite poor. The current standard of care is systemic chemotherapy with cisplatin-based regimens. These come with potential toxicities and many patients will go on to fail treatment.
Immunotherapies and immune-checkpoint inhibitors are the newest class of agents to be approved for patients who have failed cisplatin-based chemotherapy, with promising results in a subset of patients, some with durable response. However, with ~15-20% response rate and OS of ~10 months, it is not the right option for all patients.
Newer agents targeting other actionable targets are needed and many are in development. One, in particular, is erdafitinib (ERDA). ERDA is an FGFR inhibitor with activity in patients with mUC and FGFR alterations (FGFRalt). ERDA is a pan-FGFR inhibitor targeting all 4 receptor subtypes.
FGFRalt occur very commonly in non-muscle-invasive bladder cancer (NMIBC) (~40-70%) but are also found in 15-20% of mUC and are enriched in immunologically “cold” luminal type 1 UC – based on recent molecular classification schemes for MIBC. Basal type UC tend to be more aggressive but chemo-responsive.
Two independent published reports showed a 5% investigator-reported response rate to prior immune checkpoint inhibitors (ICI) among patients with select FGFRalt, suggesting that these patients would not be good candidates for ICI second-line therapy. ERDA may be able to fill this gap.
The inclusion criteria for this global, open-label phase II study was measurable mUC with prespecified FGFRalt, ECOG 0-2, and progression during/following ≥ 1 line of prior chemotherapy or ≤ 12 mos of [neo]adjuvant chemo, or were cisplatin ineligible, chemo naïve. Prior ICI treatment was allowed.
- It should be noted that patients with FGFR amplification were NOT included in the study
- This was based on initial phase 1 randomized data that assessed dosing. Continuous dosing was established to be better than intermittent dosing. They also found that higher 8 mg dosing (compared to original 6 mg dosing) was tolerable and more effective.
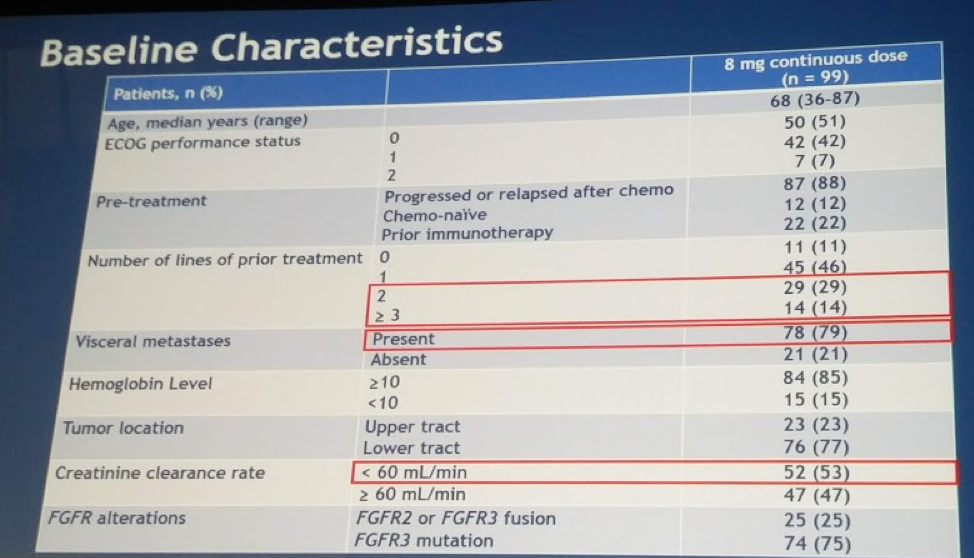
As part of this phase II study, they treated 99 pts with median 5 cycles of optimized ERDA dose regimen. Of these, 12% were chemo naïve, 43% had received ≥ 2 prior lines of therapy, 79% had visceral metastases. Creatinine clearance was < 60 in 53% of patients. Full demographics listed below:
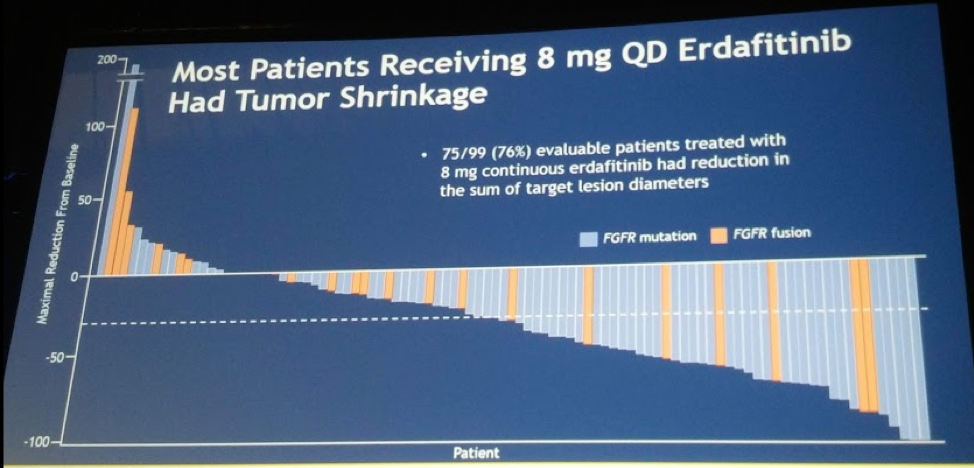
From an efficacy standpoint, there was a 40.4% confirmed ORR by RECIST 1.1 criteria (3% CR, 37.4% PR) and 79.8% disease control rate (CR + PR + SD). In particular, based on the theory above, there was a 59% ORR among pts with prior ICI (n = 21) – and only one of these patients had actually previously responded to ICI.
Waterfall plot demonstrates the degree of response:
In general, responses were early, within first 1-2 months. In terms of PFS and OS:
- PFS: Median PFS 5.5 months
- OS: Median OS 13.8 months
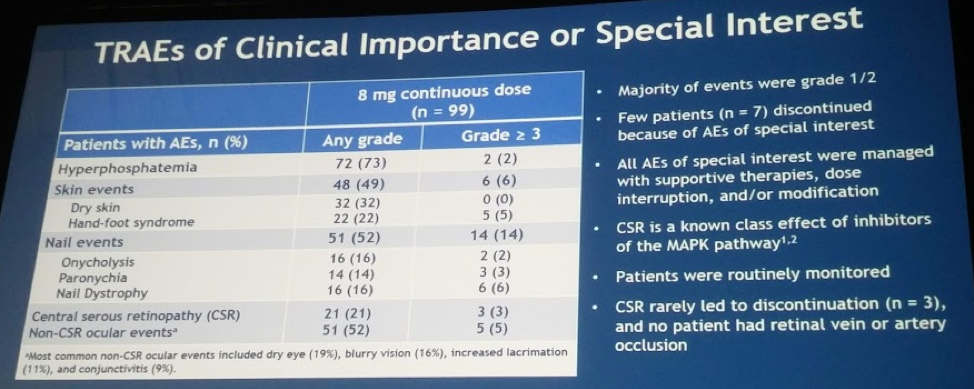
Hyperphosphatemia was the most common AE – but it was something the investigators were aiming for!
Siefer-Radtke did highlight one unique side effect profile associated with class effect of MAPK pathway targeting agents: central serous retinopathy (CSR). Patients were monitored closely for this – but very rarely was it a Grade 3 AE requiring drug cessation (3 patients, 3%).
This is a promising new therapy especially for patients who are ICI failures. Treatment with ERDA yielded a robust response rate and had a tolerable AE profile. Patients with FGFR alterations should be considered for therapy.
** It has already been given FDA approval as a Breakthrough Therapy Designation in March 2018 **
This is the phase II trial. A phase 3 clinical trial (THOR) is already ongoing, comparing erdafitinib to 2nd line chemotherapy or pembrolizumab. Phase 1b/2 NORSE trial is combining ERDA with PD-1 inhibitor. Clinical Trial: NCT02365597
Presented by: Arlene O. Siefker-Radtke, MD, The University of Texas MD Anderson Cancer Center
Co-Authors: Andrea Necchi, Se Hoon Park, Jesús GarcÃa-Donas, Robert A Huddart, Earle Frederick Burgess, Mark T. Fleming, Arash Rezazadeh, Begona Mellado, Sergei Varlamov, Monika Joshi, Ignacio Duran, Scott T. Tagawa, Anne OHagan, Anjali Narayan Avadhani, Bob Zhong, Peter De Porre, Yohann Loriot, on behalf of the BLC2001 Study Group
Author Information: The University of Texas MD Anderson Cancer Center, Houston, TX; Istituto Nazionale dei Tumori, Milan, Italy; Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South); Clara Campal Comprehensive Cancer Center (CIOCC), Madrid, Spain; Institute of Cancer Research, Sutton, United Kingdom; Levine Cancer Institute, Carolinas HealthCare System, Charlotte, NC; Virginia Oncology Associates, US Oncology Research, Norfolk, VA; Norton Healthcare, Louisville, KY; Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain; Altai Regional Cancer Center, Barnaul, Russia; Penn State Cancer Institute, Hershey, PA; Hospital Universitario Marques de Valdecilla, Santander, Cantabria, Spain; Division of Hematology & Medical Oncology, Meyer Cancer Center, Department of Urology, Weill Cornell Medical College & New York-Presbyterian Hospital, New York, NY; Janssen Research & Development, Spring House, PA; Janssen Research & Development, Beerse, Belgium; Institut Gustave Roussy, Villejuif Cedex, France
Written by: Thenappan Chandrasekar, MD, Clinical Fellow, University of Toronto, Twitter: @tchandra_uromd at the 2018 ASCO Annual Meeting - June 1-5, 2018 – Chicago, IL USA
Read a Review on Abstracts 4503-4505 by Andrea B. Apolo, MD Nonimmunotherapy Strategies in Advanced Bladder Cancer