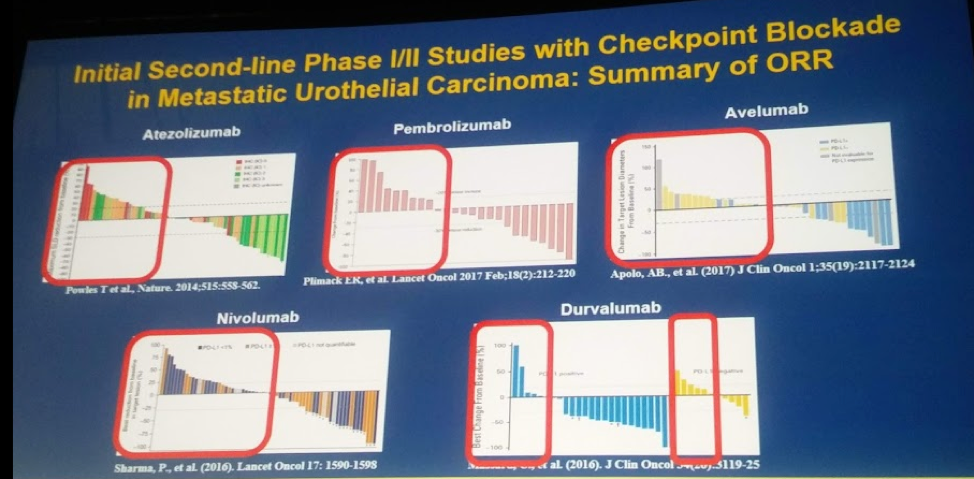
First, Apolo reiterated what all three presenters had previously noted: Despite 5 immune-checkpoint inhibitors (ICI) being approved in the 2nd line setting for patients with mUC who have failed platinum-based chemotherapy, with an objective response rate between 15-20% and OS ~10 months, there is a significant population of patients that do NOT benefit from ICI’s (highlighted in red).
She then reviewed each of the three abstracts in the following context: Does this agent add to the current standard of care? To do so, she addressed three components:
1. Clinical activity
2. Tolerable toxicity to continue drug?
3. Is there a potential for combinations to increase efficacy.
Importantly, she compared each study to Keynote-045, a phase III study of pembrolizumab vs SOC 2nd line chemotherapy (taxane or vinflunine), to highlight each drug’s efficacy in this disease space. I will present those slides to highlight her points.
First, she reviewed abstract 4505 presented by Srikala S. Sridhar, MD on Nab-paclitaxel. Unfortunately, this was essentially a negative study – no significant difference between Nap-P and paclitaxel.
1. Clinical activity – ORR 21%, median PFS 3.3 months, median OS 7.4 months.
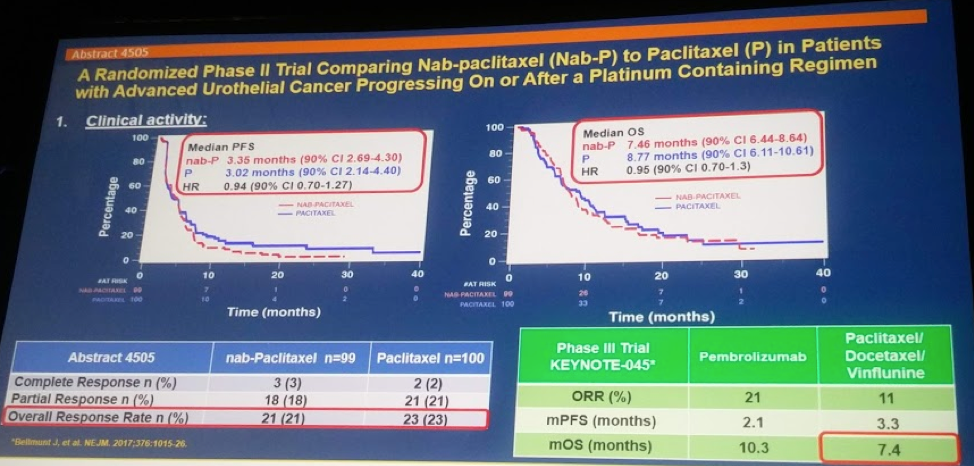
2. AE profile – it has worse AE profile that paclitaxel. 66% Grade 3-5 AE rates.
3. Combination potential – yes. Limited, but can be combined with other chemotherapeutic agents similar to paclitaxel.
- She also noted that since it doesn’t need steroids, its combination with ICI’s may be useful.
Overall, this was a negative study and may have limited use. In the Q&A session, there was an effort to salvage it by considering alternative dosing regimens.
Next, she reviewed abstract 4503 presented by Arlene O. Siefker-Radtke, MD on Erdatifinib (ERDA). This was specifically for patients with FGFR alterations (no amplification).
1. Clinical Activity – ORR 40%, median PFS 5.5 months, median OS 13.8 months, duration of response 5.6 months
2. AE profile tolerable? Yes
- 7 patients discontinued due to AE
- Central serous retinopathy led to discontinuation in 3 patients
- Grade 3+ AE profile was acceptable
3. Combination potential
- There is lots of potential with this agent!
- Drug resistance with a single target agent is inevitable – indicated by the duration of response of 5.6 months – combining it may extend the efficacy
- Preclinical models suggest synergy with PI3K inhibitors
- Phase 1b/2 NORSE trial is assessing its efficacy in combination with an ICI
Lastly, she reviewed abstract 4505 presented by Jonathan E. Rosenberg, MD on Enfortumab Vedotin (EV). This agent was not limited by specific alterations and was able to be given in all comers.
1. Clinical activity – ORR 40% (ORR 39% in patients with liver metastases), median PFS 5.4 months, median OS 13.6 months, duration of response 5.75 months.
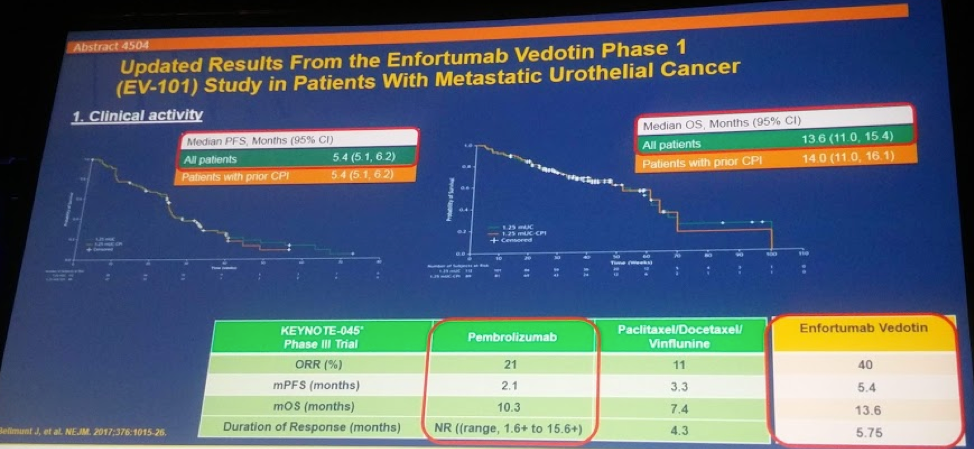
2. AE toxicity tolerable? - Yes!
- <10% had Grade 3-5 AE (no grade 5)
- 11% of patients discontinued medication due to AE’s
3. Combination potential? - YES!
- Curative chemotherapy came from combinations – so this too should be combined to increase efficacy and potentially chance of cure
- A possibility of enhancing the drug payload by attaching combination chemotherapy?
- Phase III study already ongoing combining EV with an ICI
In the discussion, one person asked if there are any biomarkers of response. At this time, no. But they are looking at it currently.
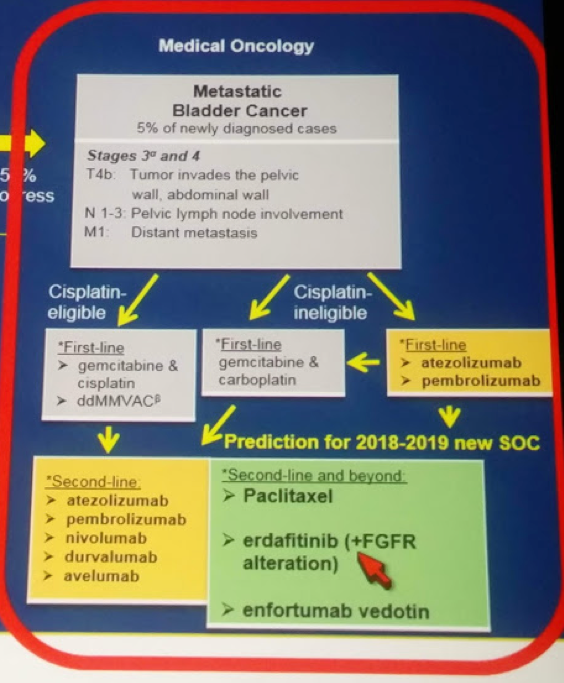
She ended by highlighting the fact that EV and ERDA have been FDA approved and the mUC disease space is finally maing some headway. Hopefully by the next year, they may become the standard of care 2nd line option after platinum-treated mUC patients.
Presented by: Andrea B. Apolo, MD, Genitourinary Malignancies Branch, Center for Cancer Research, National Cancer Institute, National Institutes of Health
Written by: Thenappan Chandrasekar, MD, Clinical Fellow, University of Toronto, Twitter: @tchandra_uromd at the 2018 ASCO Annual Meeting - June 1-5, 2018 – Chicago, IL USA