(UroToday.com) The 2024 Advanced Prostate Cancer Consensus Conference (APCCC) meeting featured a session on the management of metastatic castration resistant prostate cancer (mCRPC), and a presentation by Dr. Johann De Bono discussing which DNA repair gene alterations work for which PARP inhibitor.
Dr. De Bono started by stating that what we think we know is that prostate cancer is not one disease. Rather, it is heterogeneous, with many subtypes, including (i) inter-patient heterogeneity (even in advanced disease) leading to many trials failing because they are treating prostate cancer as one disease, and (ii) intra-patient heterogeneity (with subclones evolving over time), with this evolution leading to treatment resistance.
Importantly, prostate cancer heterogeneity cannot be ignored, particularly because prostate cancer can have various DNA repair defects. This may include germline or somatic, clonal or subclonal, and involving different parts of the DNA repair kit (bi-allelic loss means loss of function):1-2
We also think we know that the PARP enzyme is key to repairing DNA breaks. PARP is involved in double-strand DNA repair and helps ‘glue’ DNA breaks back together, thus PARP inhibition causes DNA damage. PARP inhibitors cause synthetic lethality with certain tumor DNA repair defects, killing tumor cells without both gene alleles (bi-allelic loss), sparing normal cells with both alleles and those with one allele in germline carriers. There are many genes associated with PARP inhibitor sensitivity, with BRCA1/BRCA2 loss being the first example. Other genes, include HRD genes (ie. BRCA2, PALB2), other DNA repair genes (ie. ATM, which is not an HRD gene), Fanconi anemia genes (ie. FANCA), and ribonucleotide excision genes (ie. RNASEH2B):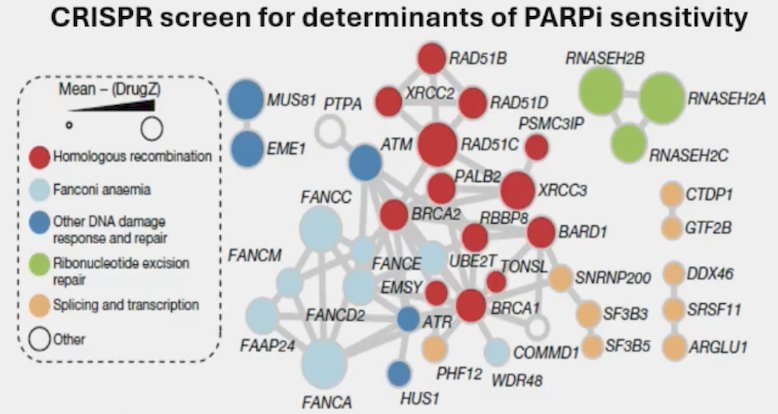
Loss of gene function is usually needed ie loss of both gene alleles.
Dr. De Bono notes that we have to deal with the complexity of DNA repair defects in prostate cancer. Some genes like BRCA2 commonly have bi-allelic loss, with homozygous deletions harder to detect. Other gene alterations like ATM are complex, given that these are large genes with many variants of unknown (functional) significance, have rare homozygous deletions, and mutations/variants are often without loss of the other allele. Further, alterations may not inform on the function leading to the study of HRD signatures (ie. archeological scars), however, HRD signatures have been less helpful in mCRPC than in ovarian cancer (mainly BRCA1 loss).
Dr. De Bono stated that we already know about BRCA gene mutations in prostate cancer and PARP inhibitor clinical antitumor activity, so he chose to focus on several less common mutations. PALB2 is BRCA2 associated and its loss potently sensitizes to PARP inhibitors. ATM bi-allelic loss can also result in PARP inhibitor responses. RNASEH2B loss is understudied, usually subclonal, and potentially sensitizes to PARP inhibitors. Looking at the TOPARP trial,3 bi-allelic PALB2 deleterious mutations had a response to olaparib, whereas mono-allelic loss did not: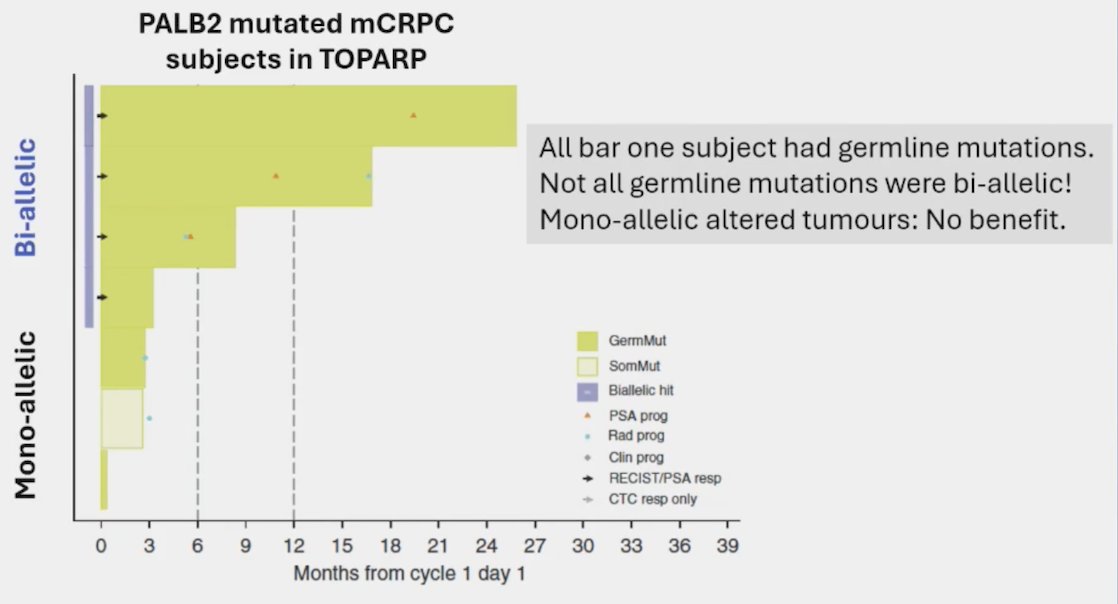
For talazoparib in mCRPC, bi-allelic loss is not mandated in ATM/PALB2 noting that there are responses to talazoparib in this setting: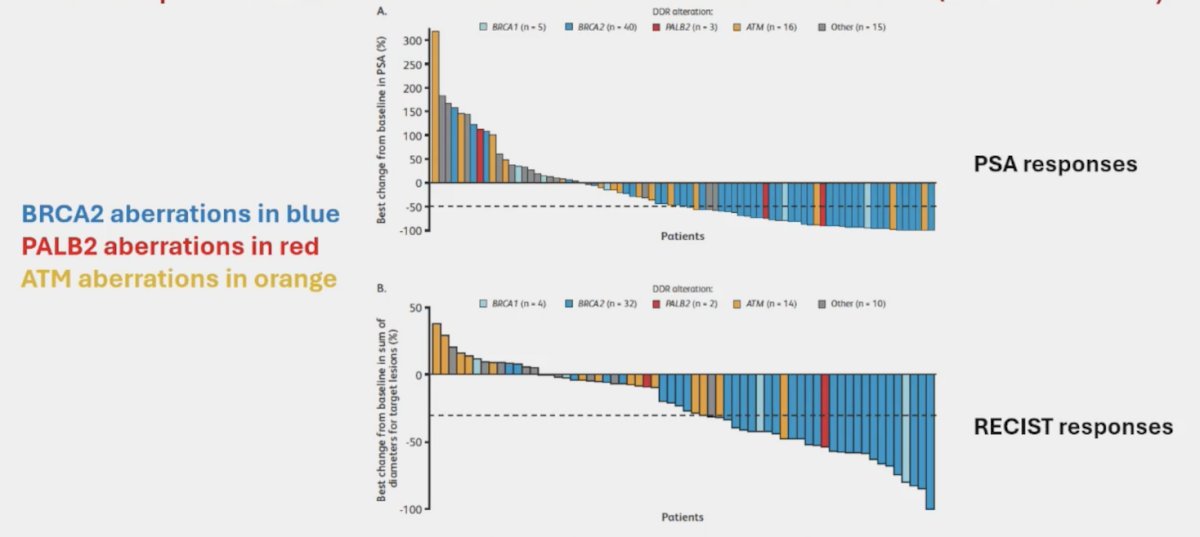
Moreover, bi-allelic loss was also not mandated in PROfound single agent phase 3 trial of olaparib.
Dr. De Bono then discussed what else we need to know. This includes needing to see overall survival benefits in relevant “non-HRD” subgroups. For example, in PROpel4 assessing abiraterone + olaparib versus abiraterone + placebo, we have not yet seen an overall survival benefit in these trials against prostate cancers without DNA repair defects: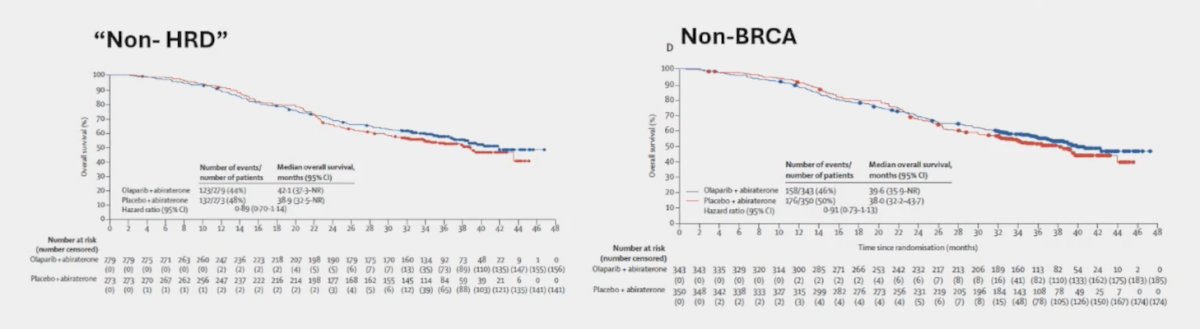
As follows is the corresponding data from PROpel looking at HRD loss and BRCA loss, with the HRD data looking worse than the BRCA data at least in part because bi-allelic loss was not mandated, according to Dr. De Bono: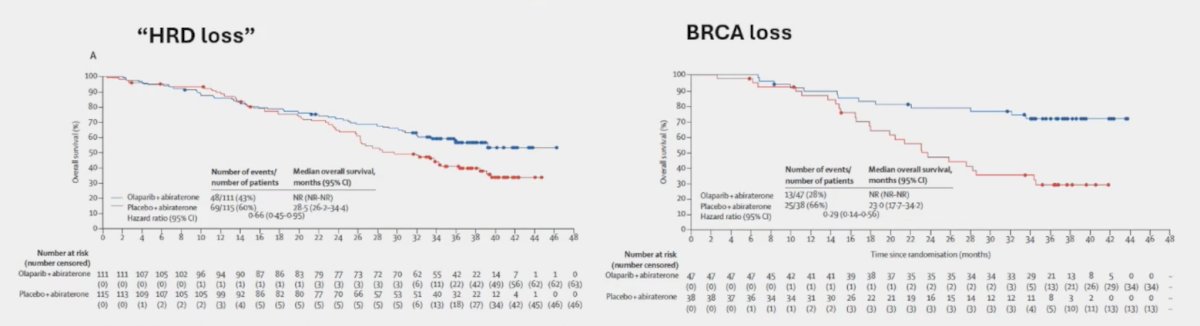
Next, we need to fully elucidate biomarker assay performance, given that PARP inhibitor clinical trial biomarker tests have major limitations:
- Is there a false positive biomarker result?
- They have not requested evidence for loss of (gene) function
- Many mutations may not result in loss of function
- They have largely not mandated bi-allelic loss
- Is there a false negative biomarker result?
- There is substantial false negative risk (ie. BRCA2 HOMDEL missed)
- Secondary to poor DNA preservation/low tumor content/tissue fraction
What we also need to know is whether PARP inhibitors induce myelodysplastic syndrome and acute myeloid leukemia and whether we need to limit PARP inhibitor duration. A recent meta-analysis assessed myelodysplastic syndrome and acute myeloid leukemia in patients treated with PARP inhibitors.5 Among 18 randomized clinical trials (n = 7,307 patients), PARP inhibitors significantly increased the risk of myelodysplastic syndrome and acute myeloid leukemia compared with placebo treatment (OR 2.63, 95% CI 1.13-6.14, p = 0.026). The incidence of myelodysplastic syndrome and acute myeloid leukemia across PARP inhibitor groups was 0.73% (95% CI 0.50-1.07; 21 events out of 4,533 patients) and across placebo groups was 0.47% (0.26-0.85; three events out of 2,774 patients). Additionally, the median PARP inhibitor duration was 9.8 months (range: 3.6 – 17.4), and the latency period from first PARP inhibitor exposure to myelodysplastic syndrome was 17.8 months and was 20.6 months for acute myeloid leukemia.
We also need to know if clearing disease subclones by PARP inhibitors is beneficial (specifically RNASEH2B), which may require rational drug combinations in selected patients. Also, do PARP inhibitors have any other mechanism of action in prostate cancer to justify their broader use beyond DNA repair defective tumors?
Dr. De Bono emphasized that there have been “mixed-up confusion” based on the FDA and EMA’s decisions for utilization of PARP inhibitors. In the meantime, for mCRPC patients post-ARSI received in the mHSPC setting, we should pursue tumor genomic analyses, preferably of fresh tumor biopsies, and think of prostate cancer as a heterogeneous disease. Additionally, we should carefully consider molecular genomic data complexity:
- Which gene is mutated? Germline versus somatic? Will alterations likely impact function?
- Biopsy tumor fraction/content (if low HOMDELS are harder to detect)
- Aberration allele frequency (low AF alterations suggest uncommon subclones)
- Consider bi-allelic versus mono-allelic loss (comparing different gene mutations)
- Consider other molecular studies if there is uncertainty (ATM IHC/RAD51 IHC assay/HRD scores)
- Artificial intelligence of tumor H&E images will likely become impactful
Dr. De Bono concluded his presentation discussing which DNA repair gene alterations work for which PARP inhibitor with the following take-home messages:
- It is Dr. De Bono’s opinion for patients suffering from mCRPC post-ARSI that we should:
- Treat all BRCA2 loss mCRPC with PARP inhibitors or platinum-based therapy since most are bi-allelic
- Treat PALB2 biallelic loss mCRPC with PARP inhibitors or carboplatin-based therapy if PARP inhibitors are not available
- Treat ATM biallelic loss with PARP inhibitors or carboplatin-based therapy if PARP inhibitors are not available
- Treat rarer biallelic sensitizing gene loss tumors (ie. FANCA, RAD51C) in therapeutic trials of PARP inhibitors or carboplatin (although we need more data)
- CDK12 is still a conundrum, as some appear to benefit from PARP inhibitors, but may have second hits on HRD
- Treatment with platinum after PARP inhibitors probably has a low likelihood of benefit given that in BRCA/HRD mCRPC, resistance is commonly due to HRD recovery of function
Presented by: Johann de Bono, MD, MSc, PhD, FRCP, FMedSci, Royal Marsden Hospital, London, UK
Written by: Zachary Klaassen, MD, MSc - Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 Advanced Prostate Cancer Consensus Conference (APCCC) Meeting, Lugano, Switzerland, Thurs, Apr 25 - Sat, Apr 27, 2024.
References:
- Mateo J, Carreira S, Sandhu S, et al. DNA-Repair defects and olaparib in metastatic prostate cancer. N Engl J Med. 2015;373(18):1697-1708.
- Pritchard CC, Mateo J, Walsh MF, et al. Inherited DNA-Repair gene mutations in men with metastatic prostate cancer. N Engl J Med. 2016;375(5):443-453.
- Mateo J, Porta N, Bianchini D, et al. Olaparib in patients with metastatic castration-resistant prostate cancer with DNA repair gene aberrations (TOPARP-B): a multicentre, open-label, randomized, phase 2 trial. Lancet Oncol 2020 Jan;21(1):162-174.
- Saad F, Clarke NW, Oya M, et al. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomized, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108.
- Morice PM, Leary A, Dolladille, et al. Myelodysplastic syndrome and acute myeloid leukemia in patients treated with PARP inhibitors: A safety meta-analysis of randomized controlled trials and a retrospective study of the WHO pharmacovigilance database. Lancet Haematol. 2021 Feb;8(2):e122-e134.
Related Content: