(UroToday.com) The 2024 Advanced Prostate Cancer Consensus Conference (APCCC) held in Lugano, Switzerland between April 25th and 27th was host to PSMA for Diagnostic and Treatment session. Dr. Ken Herrmann delivered a state-of-the-art lecture discussing next-generation prostate radioligand therapies and theranostics.
Prostate-specific membrane antigen (PSMA) is a transmembrane protein expressed by the epithelial cells lining the proximal renal tubules, salivary glands, small bowel, as well as the prostate. Expression of this transmembrane protein is upregulated in prostate cancer cells by up to a 1000-fold. The PSMA gene is located on the short arm of chromosome 11 in a region that is not commonly deleted in prostate cancer, thus making it highly prevalent in all forms of prostate cancer, including some castrate-resistant forms. Importantly, the relatively poor expression of PSMA in other organs allows for enhanced targeted imaging in prostate cancer patients.1
The radiotracers most commonly evaluated in the PSMA PET/CT setting are 68Ga-PSMA-11 (t½: 68 minutes) and 18F-DCFPyL (t½: 110 minutes), with additional radiotracers including PSMA-617, PSMA-1&T, PSMA-1007, and rhPSMA-7.68Ga PSMA-11 was FDA approved in December 2020for the initial staging of prostate cancer patients at high risk of metastases and in those with suspected recurrence based on elevated serum PSA levels. This was followed by the FDA approval of 18F-DCFPyL (Pylarify®)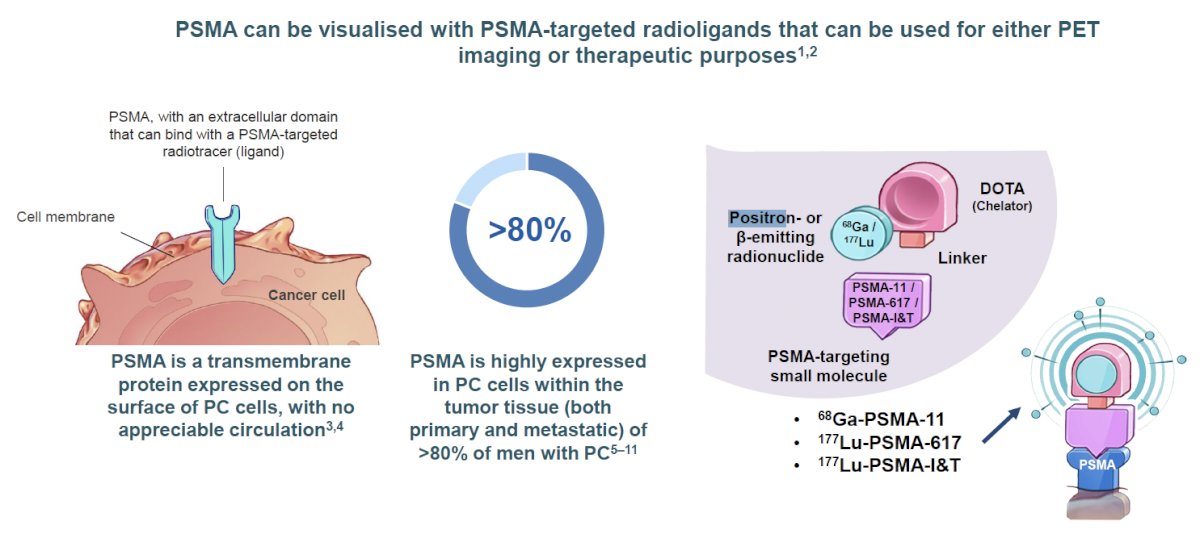
Theranostics uses the same or similar targeting agents that are labeled with either diagnostic or therapeutic radionuclides. Diagnostic radionuclides typically emit or radiation that can be read by PET/SPECT machines. Conversely, therapeutic radionuclides emit or particles that cause DNA breaks and cell damage.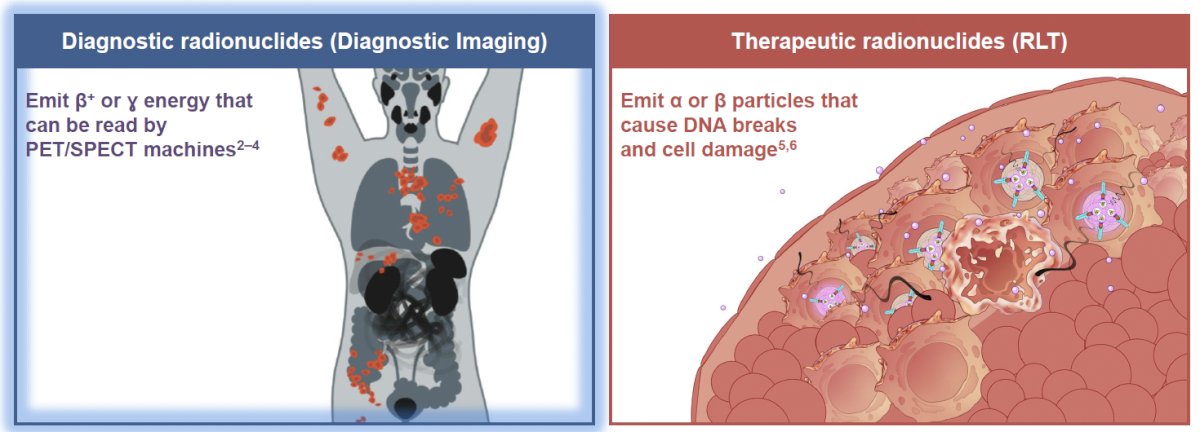
What is the ‘status’ of radioligand therapy in prostate cancer today? There are two major trials in the metastatic castrate-resistant prostate cancer (mCRPC) space that have led to the regulatory approval of 177Lu-PSMA-617 in the post-taxane and androgen receptor pathway inhibitor (ARPI) setting: VISION and TheraP.2,3
VISION is an international, open-label, phase 3 trial that evaluated 177Lu-PSMA-617 in mCRPC patients previously treated with an ARPI and 1-2 taxane regimens and who had PSMA-positive 68Ga-PSMA-PET/CT scans. Between June 2018 and October 2019, 831 patients were randomly assigned in a 2:1 ratio to receive either 177Lu-PSMA-617 (7.4 GBq every 6 weeks for four to six cycles) plus protocol-permitted standard care or standard care alone. At a median follow-up of 20.9 months, 177Lu-PSMA-617 plus standard care significantly prolonged, as compared with standard of care, both radiographic progression-free survival (median: 8.7 versus 3.4 months; HR: 0.40, p<0.001) and overall survival (median: 15.3 versus 11.3 months; HR: 0.62; 95% CI: 0.52 to 0.74, p<0.001).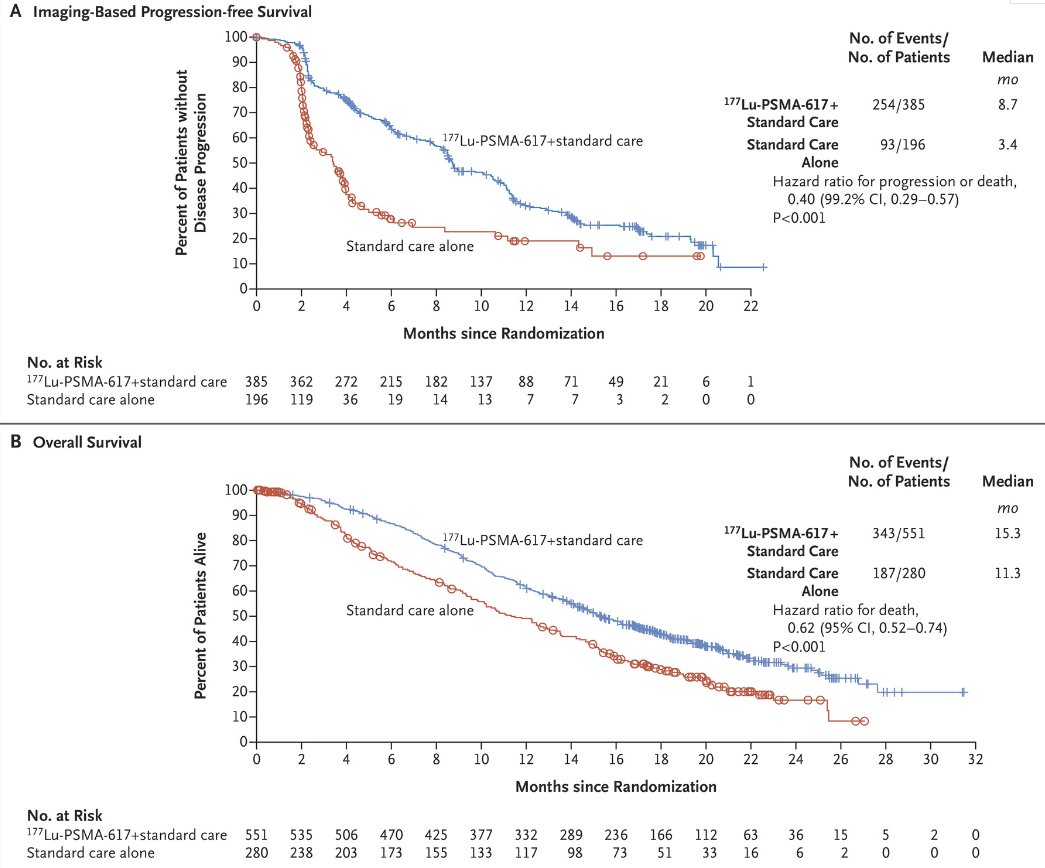
Patient-reported outcomes as evaluated by the FACT-P and Brief Pain Inventory (BPI) scores favored the LuPSMA arm with delays in time to worsening of 7.3 and 11.4 months, respectively.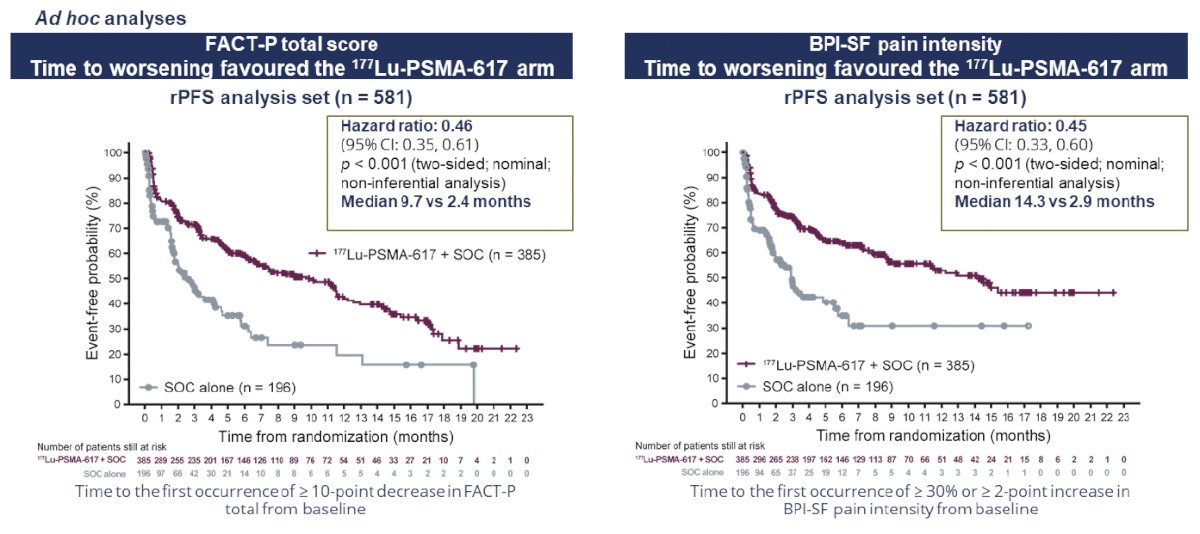
While a higher rate of high-grade (grade 3-5) treatment-emergent adverse events was observed with LuPSMA (28.4% vs 3.9%) at the time of initial reporting, overall therapy was well tolerated. It bears note that treatment exposure was more than three times longer in the LuPSMA group than in the control group.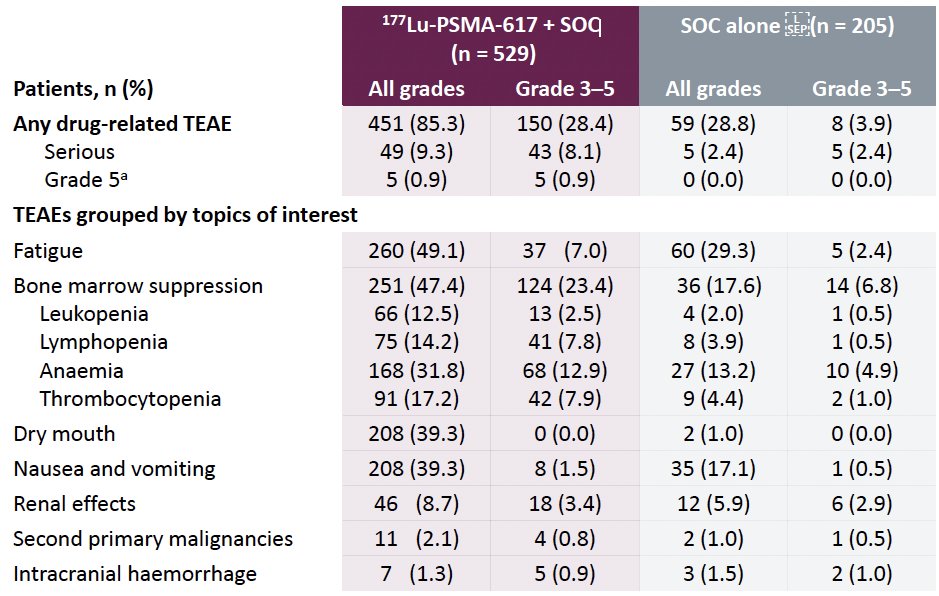
TheraP was an open-label, phase II trial of 200 mCRPC men who were randomized to either LuPSMA or cabazitaxel. To screen into the study, all men had both 68Ga-PSMA-11 and 18F-FDG PET/CT and were required to have high PSMA-expression (≥1 site with SUVmax ≥20) and no sites of FDG-positive/PSMA-negative disease. All patients had progressive disease with rising PSA ≥20 ng/mL after docetaxel and 91% had received prior enzalutamide or abiraterone. 200 patients were randomized 1:1 to LuPSMA 6-8 GBq every 6 weeks for up to 6 cycles of therapy or cabazitaxel 20 mg/m2 every three weeks for up to 10 cycles.
The most recent update of TheraP was presented at ASCO 2022 after a median follow-up of 36 months. Progression-free survival favored LuPSMA (HR: 0.62, 95% CI: 0.45 – 0.85). There was however no significant difference in overall survival between the two arms (restricted mean survival time: 19.1 months in the LuPSMA arm versus 19.6 months in the cabazitaxel arm, 95% CI for difference: -3.7 - +2.7).3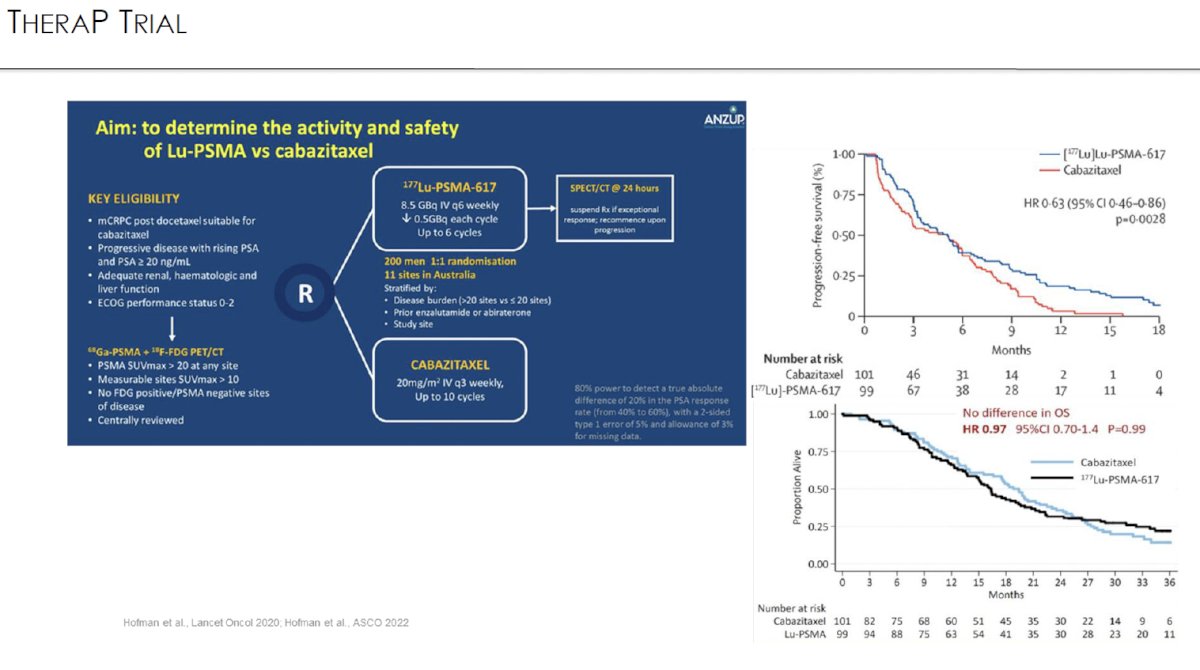
Based on the results of these trials, the current guidelines strongly recommend considering the use of 177Lu-PSMA-617 in taxane and ARPI-pre-treated mCRPC patients who have evidence of PSMA-expressing metastatic lesions as per either 68Ga or 18F-DCFPyL PSMA-PET/CT.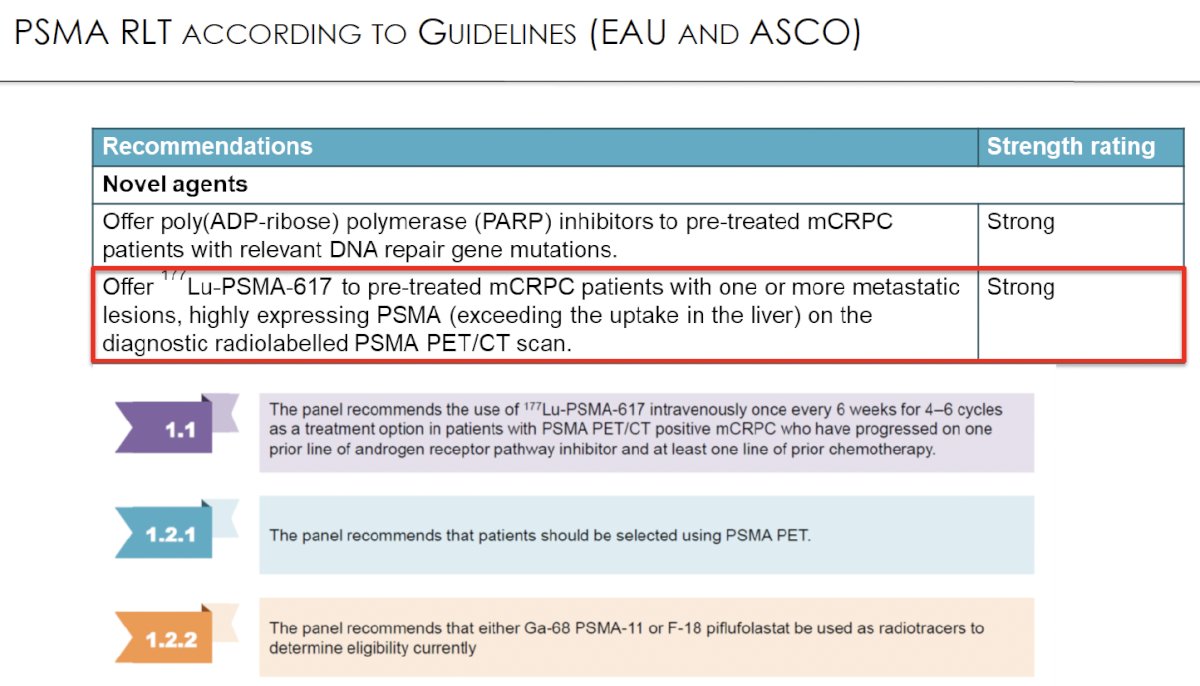
In addition to 177Lu-PSMA-617, there are numerous other radioligand therapies currently being evaluated in ongoing clinical trials.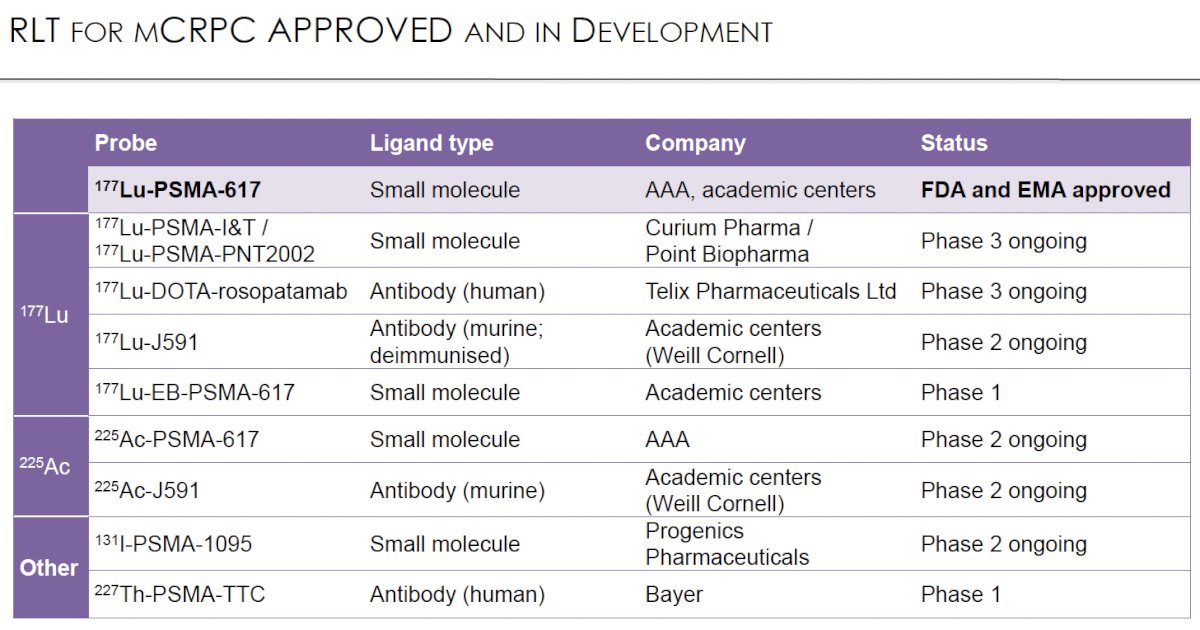
There are ongoing efforts to ‘move up’ radioligand therapy into earlier line treatment settings. SPLASH (NCT04647526) is evaluating 177Lu-PNT2002 in mCRPC patients with disease progression following an ARPI only (taxane naïve). A press release on December 18, 2023, confirmed that this trial met its primary endpoint with 177Lu-PNT2002 improving median radiographic progression-free survival from 6 months to 9.5 months (HR: 0.71, p=0.0088).4
PSMaddition (NCT04720157) is a randomized phase 3 trial evaluating the addition of 177Lu-PSMA-617 to standard-of-care therapy for men with metastatic hormone-sensitive prostate cancer.
The phase I/II LuTectomy trial is evaluating the use of 177Lu-PSMA-617 in the neoadjuvant setting prior to radical prostatectomy. Results of this trial were recently published in European Urology and demonstrated that PSA50 responses could be achieved in 9/20 patients with no observed grade 3-4 toxicities or Clavien grade 3-5 complications.5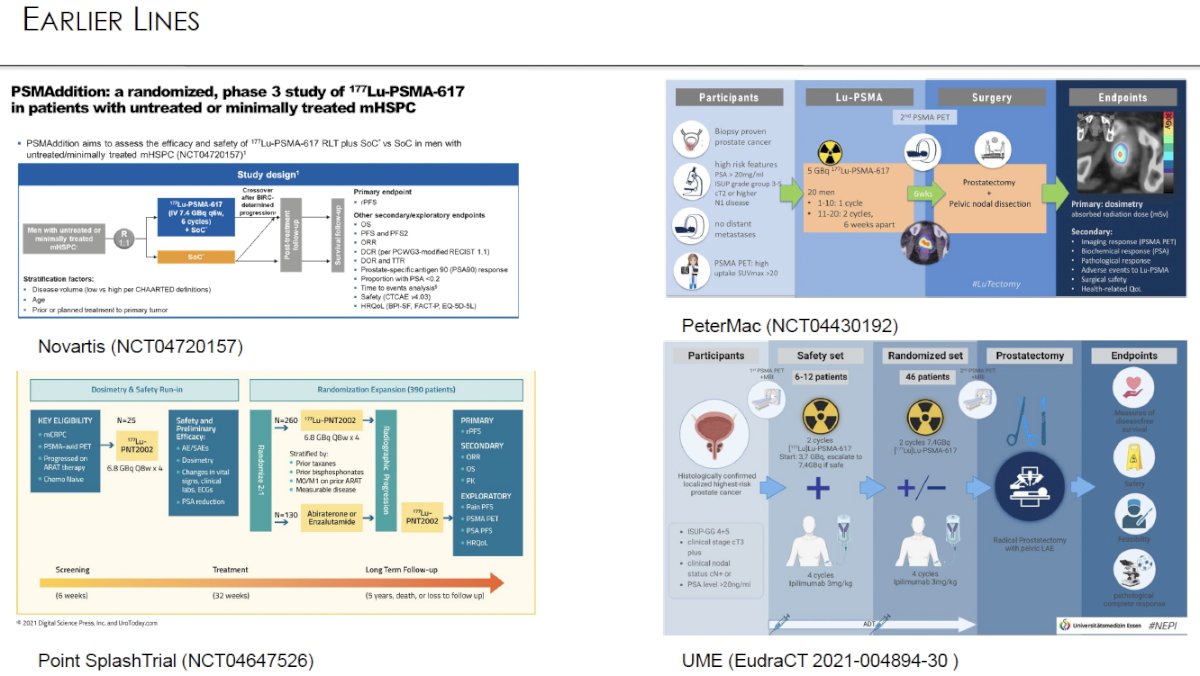
Similar to SPLASH, PSMAfore is evaluating the use of a Lu radioligand agent, 177Lu-PSMA-617, in the post-ARPI/pre-taxane mCRPC treatment setting. Interim results of this trial were presented at ESMO 2023. This is a phase III trial that randomized mCRPC patients with ≥1 PMSA positive lesion and no exclusionary PSMA negative lesions by 68Ga-PSMA-11 PET/CT 1:1 to open-label 177Lu-PSMA-617 (7.4 GBq every 6 weeks for 6 cycles) or ARPI change (abiraterone or enzalutamide). Importantly, patients randomized to ARPI could crossover to 177Lu-PSMA-617 following centrally reviewed radiographic progression. The trial design for PSMAfore is as follows: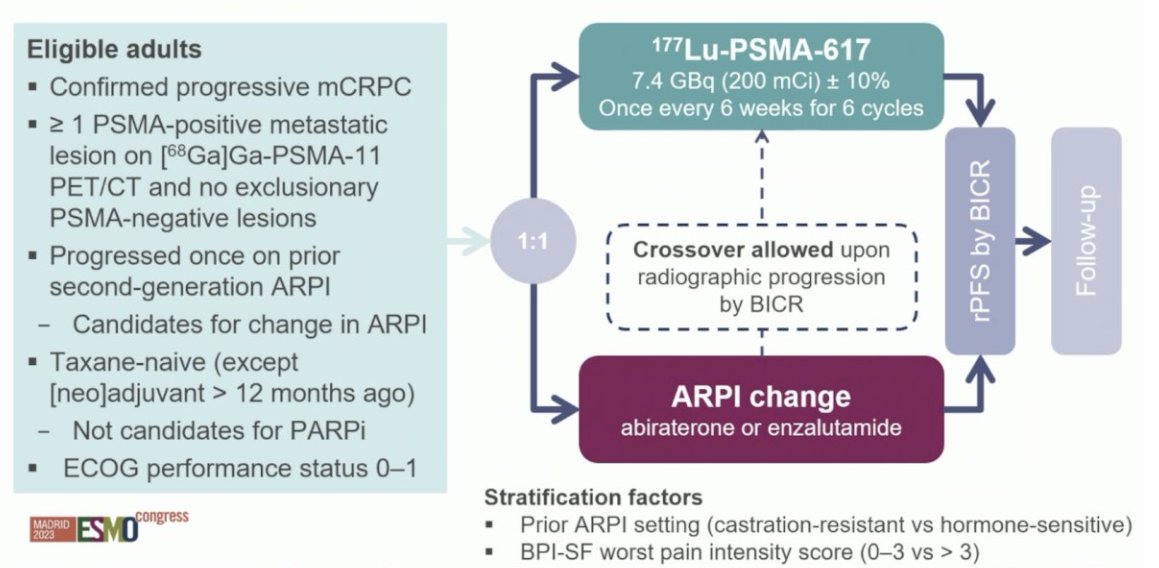
Overall, there were 468 patients randomized. At the primary analysis (median follow-up, 7.3 months), the primary endpoint of radiographic progression-free survival was met (HR 0.41, 95% CI 0.29 to 0.56), which was similar to the second interim analysis (HR 0.43, 95% CI 0.33 to 0.54). 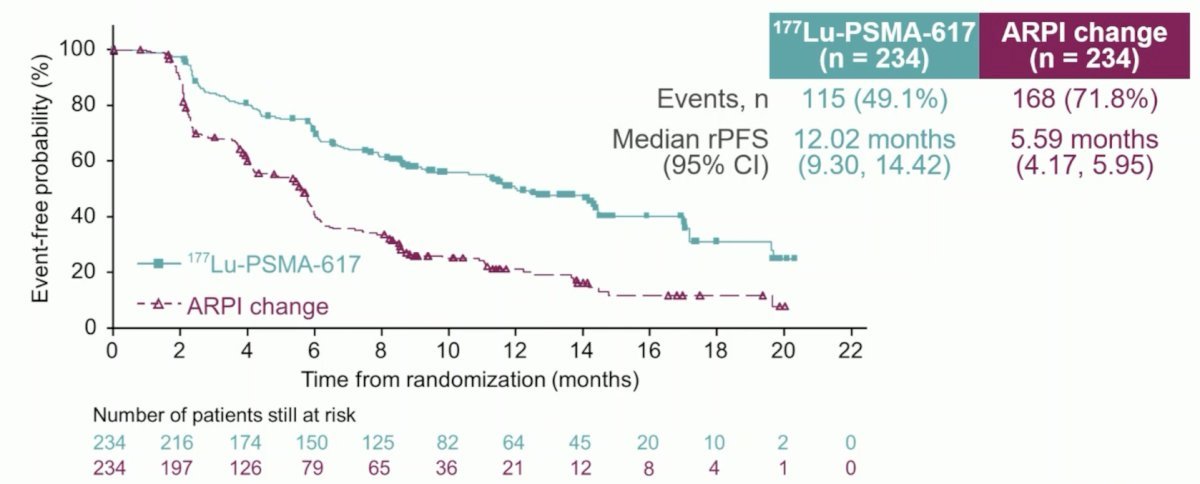
Of note, 84.2% of patients in the ARPI switch control arm who experienced radiographic progression crossed over to 177Lu-PSMA-617. In the pre-specified, crossover-adjusted overall survival data analysis, there was a non-significant overall survival benefit in favor of 177Lu-PSMA-617 (HR: 0.80, 95% CI: 0.48 – 1.33). In the unadjusted, intention-to-treat analysis for overall survival, the HR was 1.16 (95% CI: 0.83 – 1.64).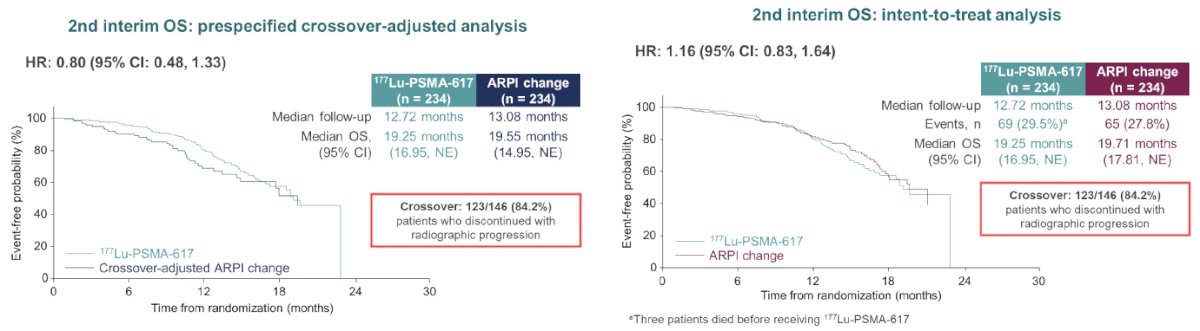
For 177Lu-PSMA-617 versus ARPI change, the incidence of grade ≥3 adverse events was 33.9% (most commonly anemia and dry mouth) versus 43.1%, serious adverse events 20.3% versus 28%, and adverse events leading to discontinuation 5.7% vs 5.2%, respectively. A summary of the most common adverse events is as follows: 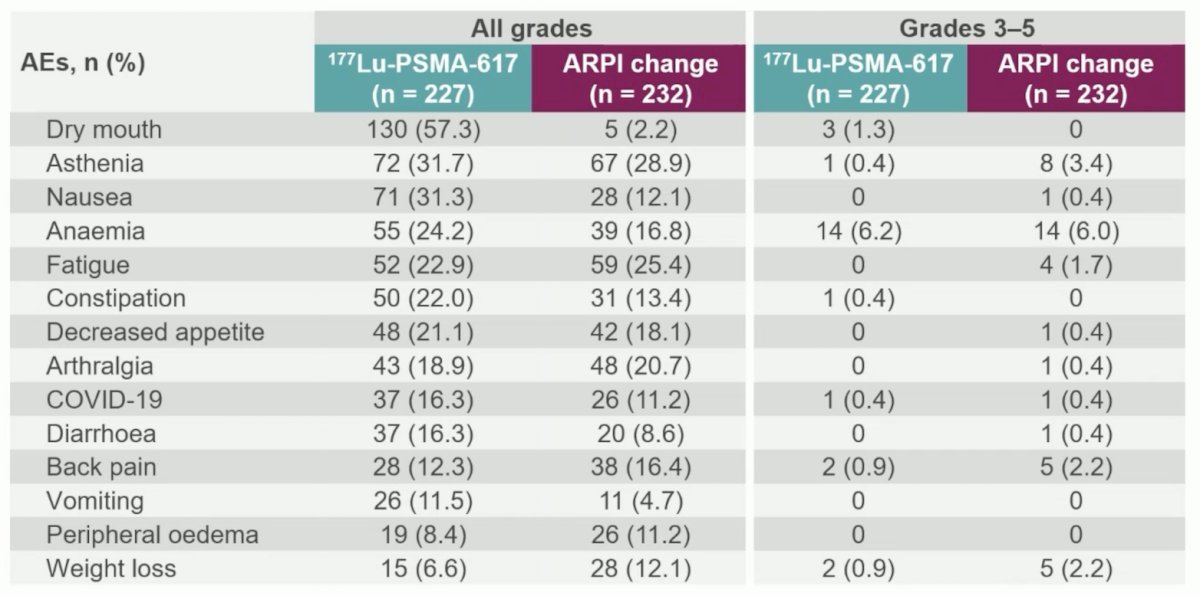
Time to symptomatic skeletal events favored the 177Lu-PSMA-617 arm (HR: 0.35, 95% CI: 0.22 – 0.57). Time to composite health-related quality of life or pain worsening as summarized by the FACT-P total score (HR: 0.59, 95% CI: 0.47 – 0.72) and BPI-SF pain intensity scale (HR: 0.69, 95% CI: 0.56 – 0.85), respectively, also favored 177Lu-PSMA-617: 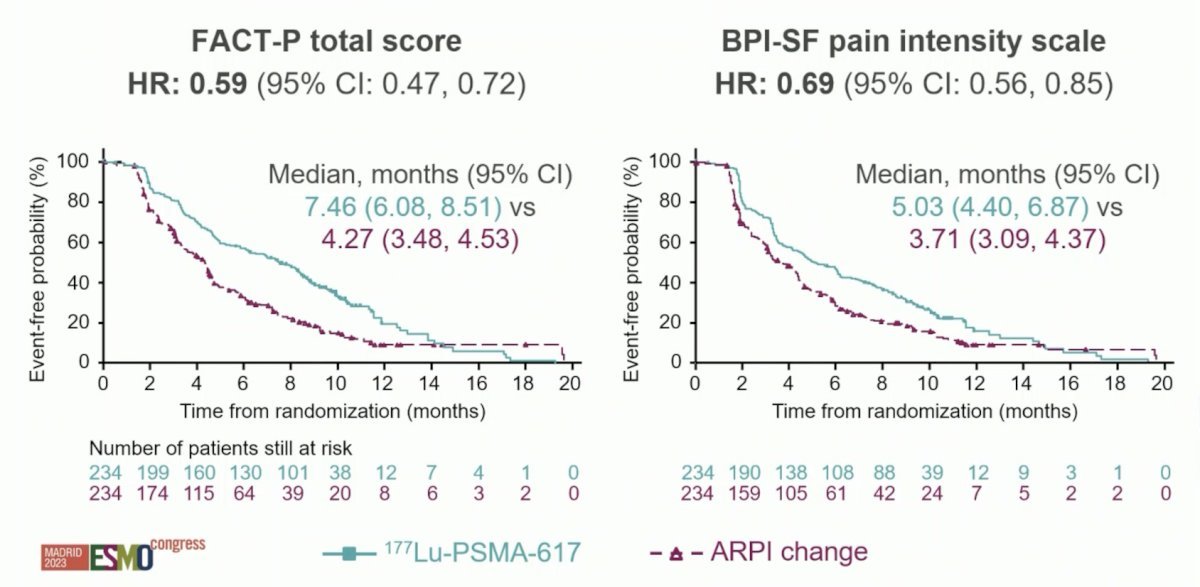
On April 4, 2024, a Novartis® press release confirmed the company’s plans to file for Pluvicto® (177Lu-PSMA-617) pre-taxane label expansion in 2024 based on updated overall survival data demonstrating a hazard ratio <1 in the unadjusted for cross-over, intent-to-treat population.
Another trial of radioligand therapy presented at ESMO 2023 was ENZA-p (ANZUP 1901), which has since been published in Lancet Oncology.6 This is an open-label, randomized phase 2 trial across 15 centers in Australia of 162 mCRPC patients who had not previously received a taxane or an ARPI in the mCRPC setting, had 68Ga-PSMA-PET/CT-positive disease, and ≥2 risk factors for early progression on enzalutamide. These patients underwent 1:1 randomization to enzalutamide +/- 177Lu-PSMA-617. 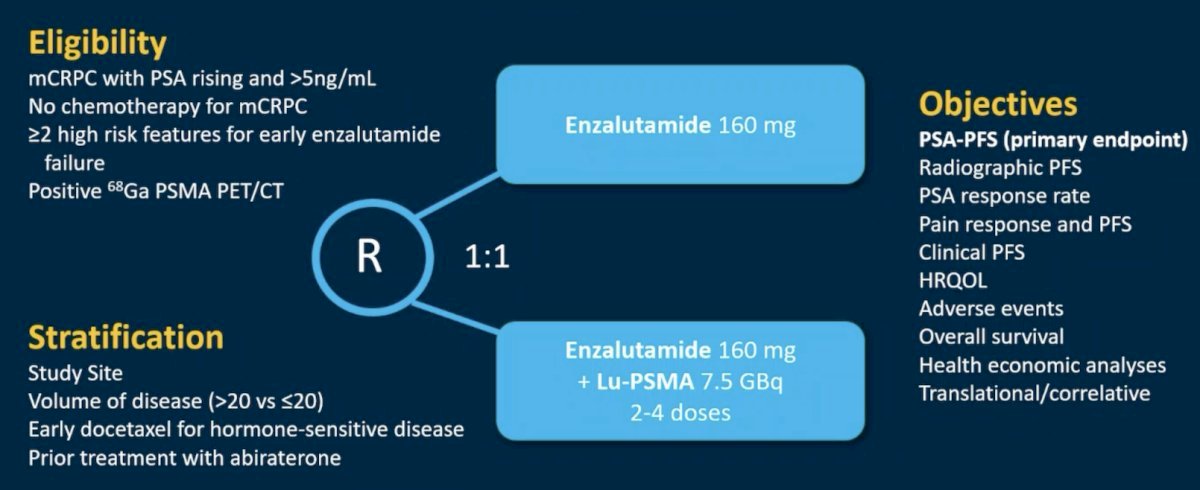
This trial met its primary endpoint, with the addition of 177Lu-PSMA-617 to enzalutamide improving PSA progression-free survival from 7.8 to 13 months (HR: 0.43, 95% CI: 0.29 – 0.63, p<0.001).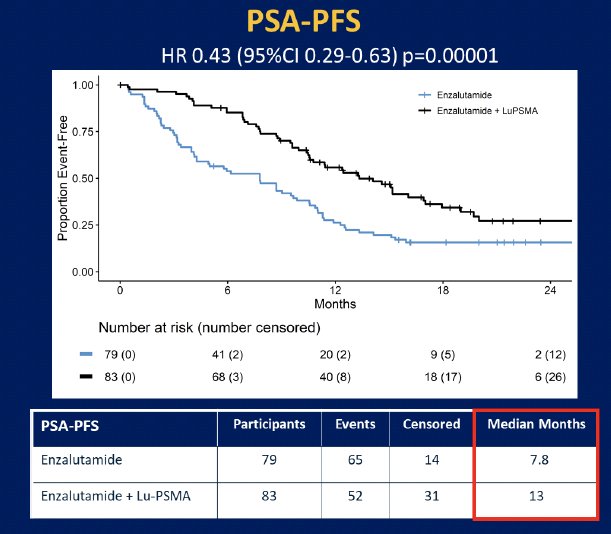
What are the ‘next generation’ targets in this space? Ideally, such agents will address areas of high unmet clinical need, including:
- Neuroendocrine differentiated tumors
- Non-PSMA expressing tumors
- Tumors with ‘inadequate’ responses to PSMA radioligand therapy
- Heterogenous tumors
There are numerous such agents currently under evaluation, as summarized in the figure below: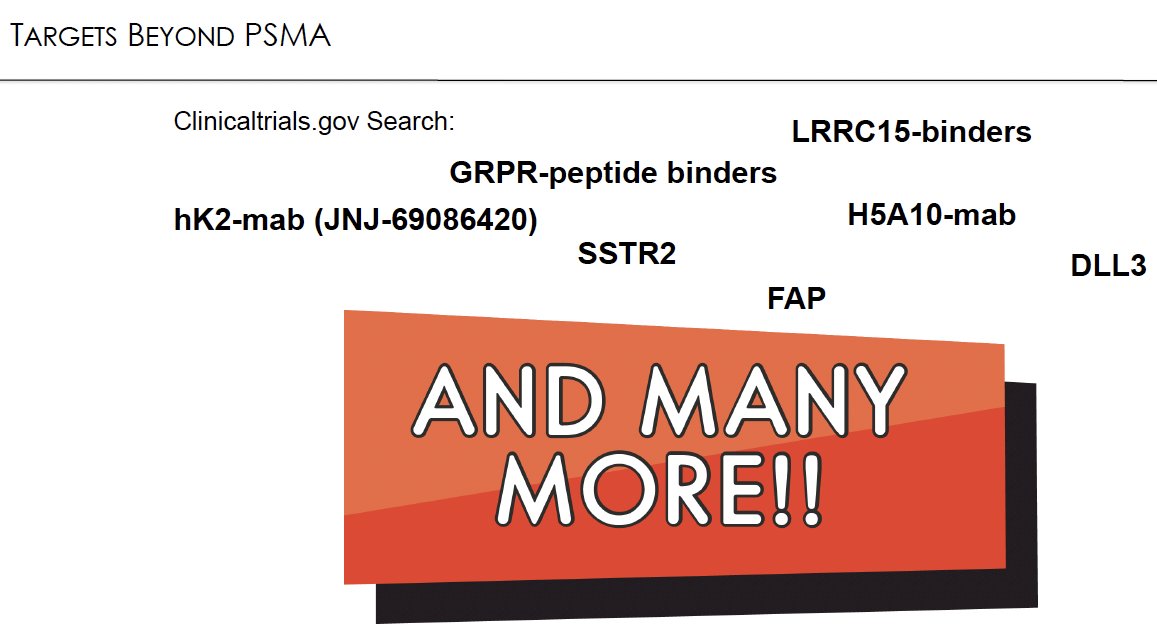
JNJ-69086420, an Actinium-225-labeled antibody targeting human Kallikrein 2 is being evaluated in a phase 1 study (NCT04644770). The expansion cohort of this trial is recruiting, with plans for initiating the phase 2 portion in 2025.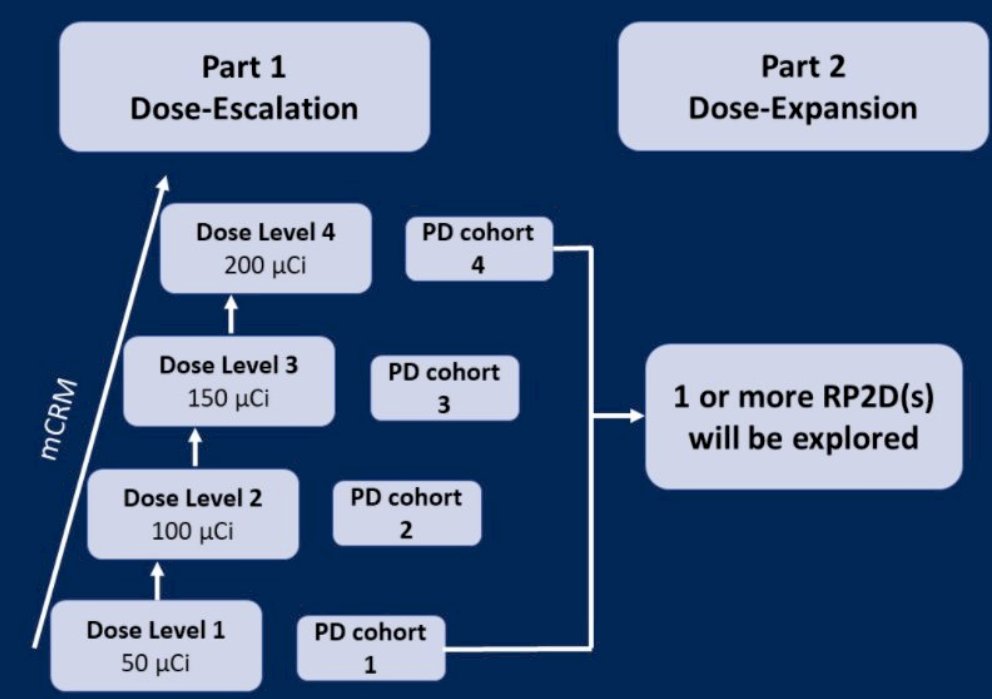
68Ga-RM2, a gastrin-releasing receptor-targeting radioligand, was compared to 68Ga-PSMA11/18F-DCFPyL for the evaluation of biochemically recurrent prostate cancer patients. Fifty patients underwent both 68Ga-RM2 PET/MRI and 68Ga-PSMA11 (n = 23) or 18F-DCFPyL (n = 27) PET/CT at an interval ranging from 1 to 60 days. 68Ga-RM2 PET was positive in 35 and negative in 15 of the 50 patients. 68Ga-PSMA11/18F-DCFPyL PET was positive in 37 and negative in 13 of the 50 patients. Both scans detected 70 lesions in 32 patients. Forty-three lesions in 18 patients were identified on only 1 scan: 68Ga-RM2 detected 7 more lesions in 4 patients, whereas 68Ga-PSMA11/18F-DCFPyL detected 36 more lesions in 13 patients. Based on these results, the investigators concluded that 68Ga-RM2 has value as a radiopharmaceutical and may have a complementary role to 68Ga-PSMA11/18F-DCFPyL PSMA PET in clinical practice.7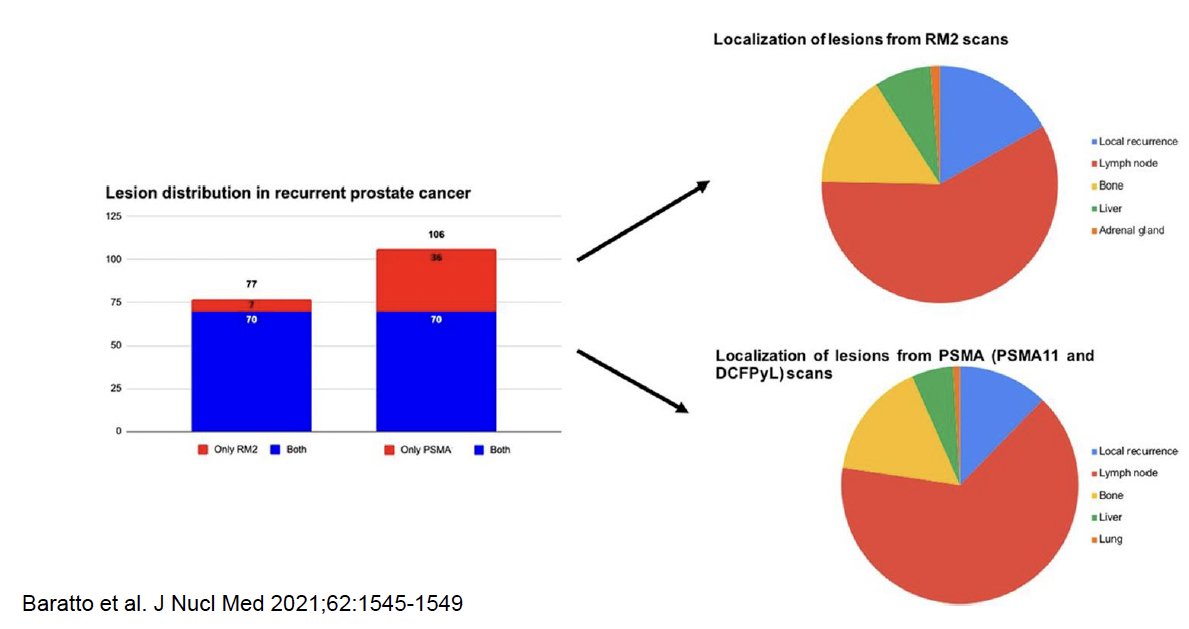
Fibroblast activation protein (FAP) is a type II transmembrane serine overexpressed in many solid cancers that can be imaged through quinoline-based PET tracers derived from an FAP inhibitor (FAPI). Given the heterogeneous nature of advanced prostate cancer with PSMA-PET/CT having limited diagnostic performance when cells are poorly expressing for PSMA, FAPI PET is being evaluated in such patients to overcome this limitation.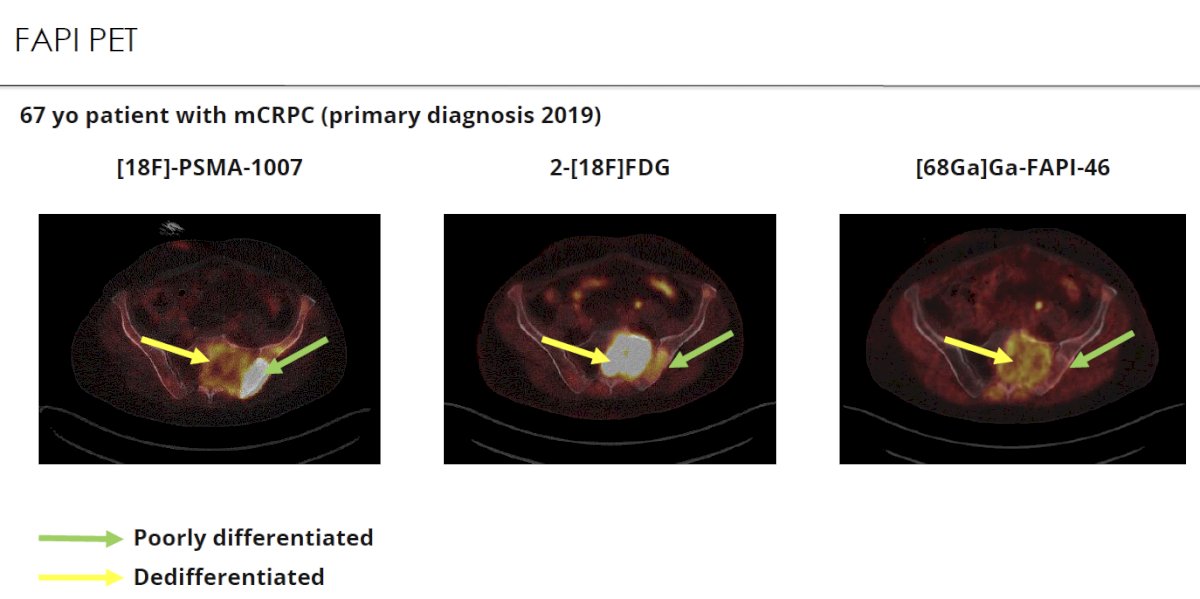
Dr. Herrmann additionally highlighted the emerging role of somatostatin receptor-2 (SSTR2) PET in this setting.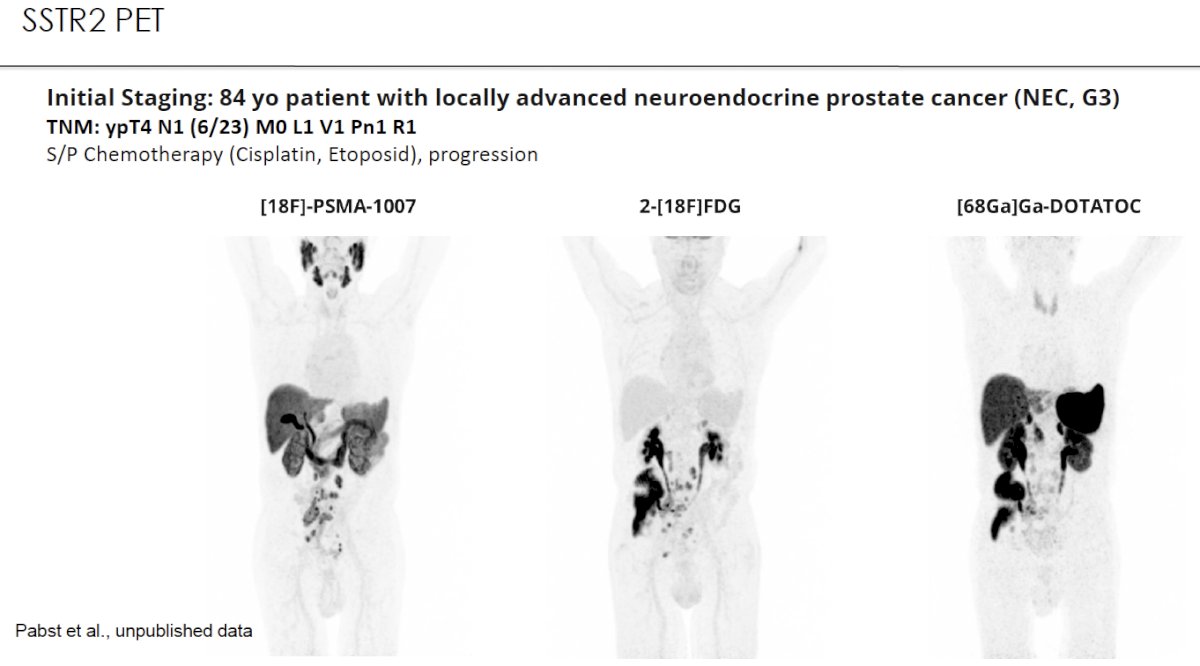
Dr. Herrmann concluded his presentation as follows:
- Theranostics involving radionuclides are ready for prime time.
- PSMA radioligand therapy is being moved up into earlier-line treatment settings
- PSMA has opened Pandora´s box in prostate cancer
- Multiple new targets are currently being evaluated
- Human Kallikrein 2 is the most advanced and closest to potential use in clinical practice
- Gastrin-releasing peptide appears to be promising in a small-group analysis
- Other targets too early to tell
Presented by: Ken Herrmann, Professor, MD, Department of Nuclear Medicine, University Hospital Essen, Essen, Germany
Written by: Rashid Sayyid, MD, MSc - Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2024 Advanced Prostate Cancer Consensus Conference, Lugano, Switzerland, April 25th - April 27th, 2024
References:- Chang SS. Overview of Prostate-Specific Membrane Antigen. Rev Urol. 2004;6(Suppl 10):S13-S18.
- Sartor O, de Bono J, Chi KN, et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021;385:1901-1103.
- Hofman MS, Emmett L, Sandhu S, et al. [177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): a randomised, open-label, phase 2 trial. Lancet. 2021;397(10276):797-804.
- Lantheus and POINT Biopharma Announce Positive Topline Results from Pivotal SPLASH Trial in Metastatic Castration-Resistant Prostate Cancer. https://lantheusholdings.gcs-web.com/news-releases/news-release-details/lantheus-and-point-biopharma-announce-positive-topline-results. Accessed on April 27, 2024.
- Eapen RS, Buteau JP, Jackson P, et al. Administering [177Lu]Lu-PSMA-617 Prior to Radical Prostatectomy in Men with High-risk Localised Prostate Cancer (LuTectomy): A Single-centre, Single-arm, Phase 1/2 Study. Eur Urol. 2024;85(3): 217-226.
- Emmett L, Subramaniam S, Crumbaker M, et al. [177Lu]Lu-PSMA-617 plus enzalutamide in patients with metastatic castration-resistant prostate cancer (ENZA-p): an open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. 2024:S1470-2045(24)00135-9
- Baratto L, Song H, Duan H, et al. PSMA- and GRPR-Targeted PET: Results from 50 Patients with Biochemically Recurrent Prostate Cancer. J Nucl Med. 2021;62(11): 1545-1549.