(UroToday.com) In the session of the 2022 Advanced Prostate Cancer Consensus Conference focusing on the treatment of patients with oligometastatic and oligoprogressive prostate cancer, Dr. Fanti presented on how to interpret and confirm lesions detected on PSMA-PET that don’t have correlates on conventional imaging.
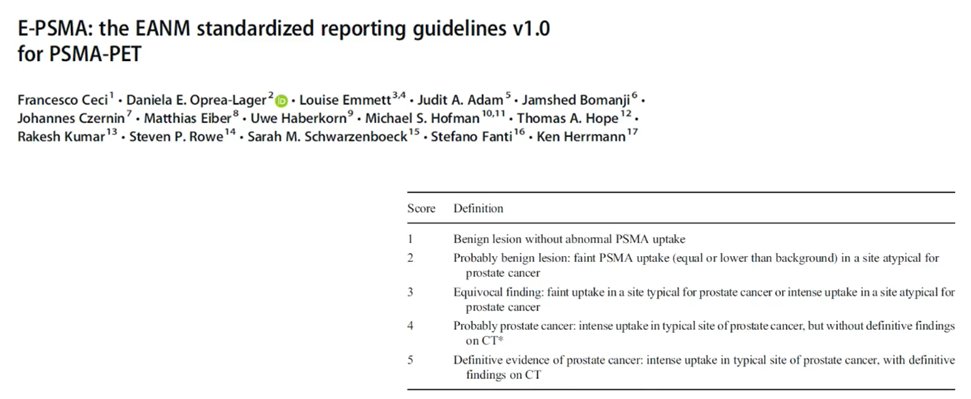
He noted first the importance of the correct interpretation of these next generation imaging studies. He emphasized the importance of adhering to reporting guidelines, such as the EANM standardized reporting guidelines for PSMA-PET (E-PSMA). These provide a rigorous and reproducible way of interpreting PSMA-PET studies with an objective scoring system.
However, he further noted that there are limitations of all imaging modalities and none will have 100% accuracy. As a result, there is often a need to confirm or refute equivocal findings. He noted that other orthogonal imaging including x-ray, CT scan, MRI, and ultrasound may be used. For uncertain lesions in the axial skeleton, he emphasized that MRI can often provide a definitive answer and resolve uncertainties. However, when the uncertainty relates to nodal disease, CT scan may be more appropriate. He highlighted specific patient imaging examples to emphasize these points. At some times, he emphasized there may be no available imaging approach that can be used to address uncertainty from the PSMA-PET. In this case, where feasible, he suggested that biopsy can be considered to help clarify diagnostic uncertainties. However, many times this is not possible. In that case, options include interval imaging to assess the evolution of disease, a therapeutic trial, or a philosophic consideration regarding the value of confirmation. Citing the example of COVID-19 testing in which we would not use a rapid antigen test to confirm a PCR based diagnosis, he emphasized that we shouldn’t use “lesser” imaging results to confirm results from a more accurate modality. Thus, as PSMA-PET has higher accuracy (particularly among patients with low PSA levels) than other imaging modalities, we should potentially simply act on the results of the PSMA-PET.

However, he acknowledged that the downfall of this approach, and the “elephant in the room”, is the false positive rate of PSMA-PET. Rates of false positives differ between different radiotracers and different interpreting nuclear medicine physicians. He noted, in particular, a risk of false positive rib lesions. In most testing scenarios in medicine, we can decrease the risk of false positives by shifting sensitivity down, at the expense of increased false negative results. It’s not clear that this would be desirable in the context of routine clinical use of PSMA-PET. Thus, he emphasized the importance of the expertise of the interpreting physician and the optimal tracer choice. He noted that PSMA is a basket concept with many different tracers utilized, each with differing properties.
He highlighted, in particular, that PSMA-1007 has non specific uptake in bone marrow which may lead to false positive bony lesions. When compared with 68Ga-PSMA-11, PSMA-1007 detected a similar number of true lesions but had a much higher false positive rate. This effect, however, may be mitigated by the expertise and familiarity of the reviewing physician. Citing again the example of solitary rib lesions, he emphasized that appropriately expert physicians can accurately identify these benign lesions and, in most circumstances, further intervention to confirm the diagnosis is not required.
However, obviously, not all rib lesions are false positives and many may represent actual sites of disease, even in the absence of correlates on conventional imaging (bone scan and CT scan). To this end, he cited a case example in which a therapeutic trial (with SBRT) confirmed the diagnosis.
Moving forward, he emphasized that PSMA-PET based imaging is a game changer in the management of patients with prostate cancer. However, ongoing work is required to ensure that this technology is maximally used for the benefit of our patients. He highlighted the value of multidisciplinary tumor boards as clinical data may often be useful in clarifying diagnoses for interpreting nuclear medicine physicians.