The case presented by Dr. Krieger was of a 71-year-old male, retired naval officer, and lawyer with a medical history including CHOP chemotherapy for lymphoma 14 years earlier, a 25-pack-year smoking history (stopped 14 years ago), and warfarin for atrial fibrillation. His performance status was excellent and he presented with gross hematuria. Dr. Krieger highlighted that the following are all risk factors for developing bladder cancer, including prior cyclophosphamide chemotherapy, smoking, increasing age, schistosomiasis, azo dye/petrochemicals/arsenic exposure, pioglitazone therapy for diabetes, and male gender. For this patient, a CT IVP demonstrated asymmetrical thickening of the left bladder wall, and cystoscopy showed multifocal areas of erythema plus a visible papillary lesion close to, but not involving the ureteral orifice. Subsequent TURBT showed CIS with high-grade T1 papillary urothelial carcinoma, with muscle present in the resection specimen, but not involved with tumor. The following next steps in management options were then presented to the audience: (i) check cystoscopy at 4-6 weeks with re-resection, (ii) Bacillus Calmette-Guerin (BCG) induction therapy, (iii) intravesical mitomycin, (iv) intravesical nadofaragene firadenovec, or (v) cystoscopy surveillance alone. 50% of the audience favored a cystoscopy with re-TURBT in 4-6 weeks, and 40% BCG induction therapy.
Next, the patient underwent re-resection of his tumor bed, which was clear of residual disease. He was then randomized to the standard BCG arm of the ANZUP BCG/mitomycin trial and completed six doses of BCG over an eight-week period (2 delays secondary to hematuria and a UTI). Cystoscopy surveillance at 3 months showed a single focus of low-grade non-muscle-invasive bladder cancer (NMIBC), which was resected; additional BCG granulomatous changes were seen visually and on histology. At this point the audience was given the following options for the next steps in management: (i) cystectomy, (ii) BCG re-induction, (iii) proceed with maintenance BCG therapy, (iv) re-induction with intravesical chemotherapy, or (v) surveillance alone. As follows is the results of this poll: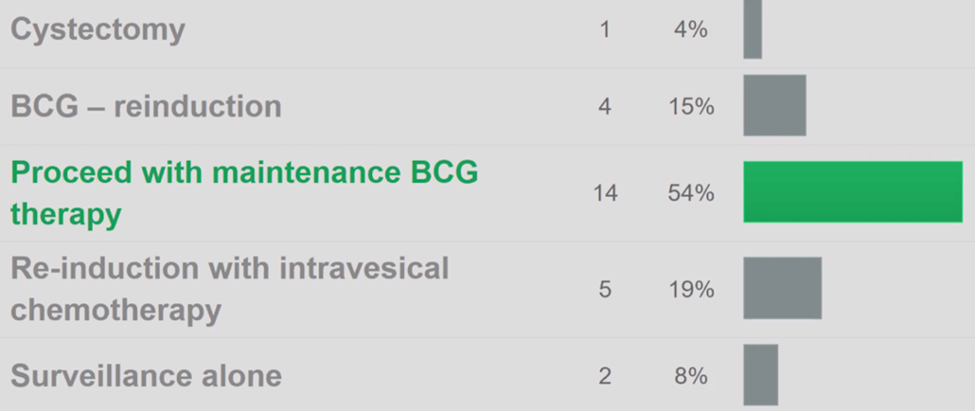
The patient ultimately completed 10 months of maintenance monthly BCG therapy, with cystoscopy 3-4 months remaining negative. At 20 months after his initial diagnosis he had recurrent hematuria, a decline in renal function (eGFR 50 ml/min), however, his cystoscopy two months prior was unremarkable. He subsequently underwent a CT that showed unilateral hydronephrosis with mid-ureteric thickening and no obvious lymphadenopathy. A cystoscopy with ureteroscopy showed no evidence of disease in the bladder, but an obstruction at the mid-ureter that was biopsy-proven high-grade papillary urothelial carcinoma. The following options were then provided to the audience, including (i) nephroureterectomy, (ii) pembrolizumab, (iii) neoadjuvant chemotherapy, (iv) definitive chemo-radiotherapy, or (v) re-challenge intravesical BCG therapy. Given that staging for upper tract urothelial carcinoma is challenging both the panel and the audience (71% of those polled) preferred nephroureterectomy.
The patient subsequently underwent a radical nephroureterectomy with pathology demonstrating T3N0 high-grade urothelial carcinoma with negative margins. Based on the recently published POUT trial1 showing that gemcitabine-platinum combination chemotherapy initiated within 90 days after nephroureterectomy significantly improved disease-free survival in patients with locally advanced upper tract urothelial carcinoma, both the panelists and the audience (76% of those polled) favored adjuvant platinum doublet chemotherapy for this patient.
The patient subsequently had recurrent hematuria just prior to a planned surveillance cystoscopy; a CT scan at that point showed that the remaining upper tract and kidney were normal, but there was thickening of the bladder base. Cystoscopy showed a 1.5 cm papillary lesion with several red patches, with Transurethral resection of bladder tumor (TURBT) pathology showing high-grade NMIBC plus multifocal carcinoma in situ (CIS) (muscle present but not involved). With this most recent high-grade bladder recurrence, the audience was polled and offered the following options: (i) proceed with completion cystectomy, (ii) re-challenge with BCG therapy, (iii) radiotherapy alone if ongoing bleeding or stage progression occurs, (iv) definitive chemo-radiotherapy, or (v) a trial of intravesical chemotherapy (gemcitabine or gemcitabine plus docetaxel). 29% of the audience would proceed with completion cystectomy or (29%) a trial of intravesical chemotherapy. He ultimately declined a cystectomy stating that he wanted to the ‘least invasive’ measures of reducing risk, thus he proceeded with BCG re-induction and maintenance therapy. Six months later he had further hematuria, with increased urinary frequency and urgency (eGFR now 45 ml/min). Cystoscopy and TURBT showed once again high-grade urothelial carcinoma with multifocal CIS; muscle was present and very close to tumor involvement (probably T2 – but not 100% confirmed). Next steps in management included (i) proceed directly to radical cystectomy, (ii) neoadjuvant chemotherapy, (iii) further staging including MRI +/- PET CT scan, (iv) screen for BCG refractory immunotherapy trial (ie. KEYNOTE-057, etc), or (v) definitive chemo-radiotherapy. 76% of the audience favored proceeding directly to radical cystectomy, whereas 18% of respondents would screen for a BCG immunotherapy trial. Dr. Krieger then provided the following statements that should be kept in mind when treating patients with muscle-invasive bladder cancer:
Importantly, he notes that patients who require salvage cystectomy post-chemoradiotherapy should not be routinely offered a neobladder.
This patient still declined a cystectomy and underwent chemoradiotherapy with platinum chemotherapy. From his treatment, he developed grade 1 neuropathy and grade 1 fatigue, with a stable eGFR of 40 ml/min, minimal bladder irritation, and a stable ECOG status of 0. Following definitive, there is debate as to the appropriate surveillance algorithm, as such the following options were provided to the audience: (i) 3-6 monthly MRI/PET, (ii) 3-6 monthly cytology, cystoscopy plus CT surveillance, (iii) none, relapse risk is 10% in an almost 80-year-old, (iv) renal/bladder ultrasound 3-6 monthly alone, (v) urine cytology, labs, tumor markers, and clinical examination; imaging and cystoscopy only if indicated. Overwhelmingly, 79% of respondents would opt for a 3-6 month cytology, cystoscopy, and CT surveillance. Dr. Weickhardt notes that in his practice he performs q3-6 month surveillance cystoscopy/imaging for the first two years and then extends to every six months (for cystoscopy) and every 12 months (for imaging) after two years of follow-up.
During follow-up, the patient presented again with mild anorexia and flank pain and found to have an eGFR of 20 ml/min with labs otherwise unremarkable except for a CA 19-9 level of 1200. A renal ultrasound demonstrated new hydronephrosis of the remaining kidney; cystoscopy and ureteral stenting showed evidence of radiotherapy changes within the bladder and ureteric orifice, with likely extrinsic compression of the ureter. He underwent a PET-CT which showed multiple peritoneal nodules with tracer avidity. Dr. Eade notes that there is a limited role for surgery in these patients, but for symptom control, a pelvic exenteration may be warranted in select patients. The patient ultimately received pembrolizumab with clinical improvement (weight gain, the return of appetite), and a staging CT scan showing significant response with minimal peritoneal thickening and no new disease. Dr. Krieger notes that there is no good answer as to how long immunotherapy should be continued, but typically patients are treated until disease progression or treatment toxicity.
Presented by:
Chair: Laurence Krieger, MD, Medical Oncologist, Director of Clinical Trials for the Riverina Cancer Care Centre and clinical trials clinic, Royal North Shore Hospital, Sydney, Australia
Panelists:
Venu Chalasani, MBBS, PGDip, FRACS, Urologist, Northern Beaches Hospital, Sidney, Australia
Tom Eade, MBChB FRANZCR, Associate Professor, Radiation Oncologist, Director of Research in Radiation Oncology at Northern Sidney Cancer Centre, Sidney, Australia
Andrew Weickhardt, MBBS (Hons), DMed Sc, Associate Professor, School of Cancer Medicine, La Trobe University, Medical Oncologist, Senior Clinical Research Fellow, Translational Scientist, Olivia Newton-John Cancer Wellness and Research Centre, Melbourne, Australia
Kathryn Schubach, Nurse Practitioner for the Uro-oncology Service at Peter Mac, Australian and New Zealand Urology Nurses, Melbourne, Australia
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md during the 2020 Australian and New Zealand Urogenital and Prostate Cancer Trials Group (ANZUP) Mini Annual Scientific Meeting (ASM), November 29 - 30, 2020