(UroToday.com) In a podium presentation at the 2022 American Urologic Association Annual Meeting held in New Orleans and virtually, Dr. Hu presented surgical outcomes of patients undergoing retroperitoneal lymph node dissection (RPLND) in the context of the SEMS trial.
The SEMS trial established primary RPLND as an option for treating seminoma with isolated retroperitoneal lymphadenopathy. The surgical outcomes of this contemporary, multi-institutional cohort are of value given that the existing literature on peri-operative outcomes and long-term complications of RPLND is largely retrospective, single institution and historical.
The authors reviewed surgical outcomes for patients with treatment naïve testicular seminoma and isolated retroperitoneal lymphadenopathy (1-3 cm) treated in the context of this phase II, prospective clinical trial. All patients underwent open RPLND and were seen for a post-operative visit within 30 days of surgery and then at routine intervals. History, physical, laboratory and radiographic evaluation were performed at each visit. The Clavien-Dindo system was used to classify complications within 30 days. Nerve-sparing approach was determined by operative reports and confirmed by an independent review of intra-operative photos.
The authors included 55 patients who were treated at 12 institutions with 19 different surgeons. RPLND was performed via both transperitoneal (n = 40) and midline extraperitoneal (n = 15) techniques with a median duration of surgery of 233 (IQR 178-313) minutes. A variety of templates were used including bilateral in 19 patients, left modified in 25, and right modified in= 11. Nerve-sparing within the template was performed in the majority of patients (n=48, 87%). Median blood loss was 150 (IQR 100-300) ml and no patients required intraoperative blood transfusion or within 30 days post-operatively. The median length of stay was 3 (IQR 2-4) days.
Post-operatively, patients were followed for a median of 33 (IQR 27-40) months. Four (7%) individual patients experienced five short-term complications: 1 had Clavien-Dindo grade I, 3 had grade II, and 1 had grade IIIa events.
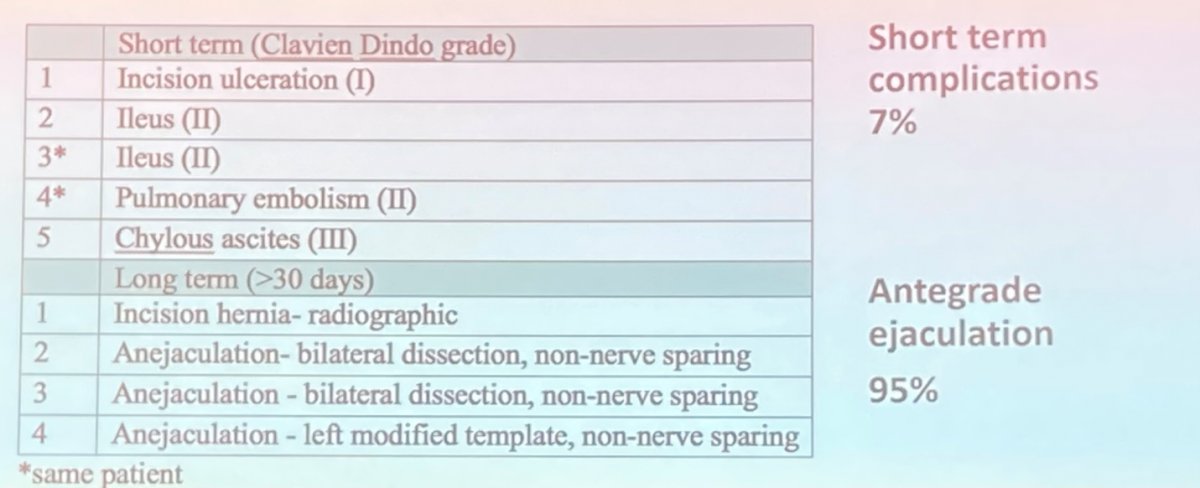
Over a longer term, six (11%) patients experienced a complications, including incisional hernia in 2 patients (one was asymptomatic and only seen radiographically) and retrograde ejaculation in 3 patients. Notably, antegrade ejaculation was preserved in 98% of patients who underwent nerve-sparing surgery.
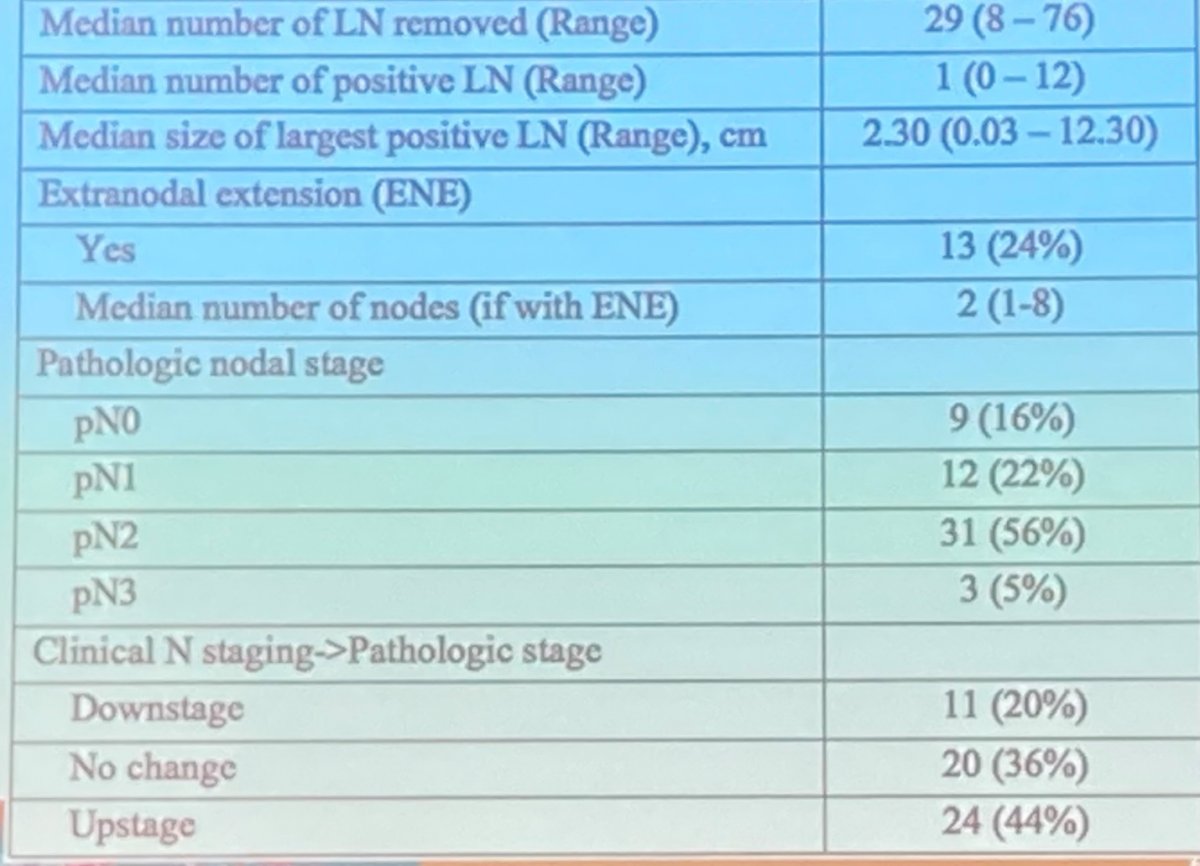
Dr. Hu further briefly mentioned pathological outcomes which from the SEMS trial have previously been reported. As highlighted below, there is a significant rate of nodal upstaging.
Following primary RPLND, the authors reported that 2 year recurrence free survival was 81%, though there were some differences in recurrence rates on the basis of pathological nodal status noted.

Presented by: Brian Robin Hu, MD – Loma Linda Urology