One such pathway involves enhancer of zeste homolog 2 (EZH2), a histone methyltransferase that has emerged as a key regulator of prostate cancer progression and therapeutic resistance. Mevrometostat, an oral, potent, and selective EZH2 inhibitor, is currently being evaluated in a comprehensive phase III clinical trial program spanning multiple stages of advanced prostate cancer. The MEVPRO program includes MEVPRO-1 in post-abiraterone mCRPC, MEVPRO-2 in ARPI-naïve mCRPC, and MEVPRO-3 in ARPI-naïve mCSPC, representing an effort to evaluate EZH2 inhibition across the entire advanced disease continuum.
EZH2 as a Therapeutic Target in Prostate Cancer
EZH2 is the catalytic component of the polycomb repressive complex 2 (PRC2) and functions as a histone methyltransferase that mediates epigenetic gene silencing through trimethylation of histone H3 lysine 27 (H3K27me3). Although EZH2 has canonical roles in chromatin remodeling and transcriptional repression, its biologic relevance in prostate cancer extends beyond epigenetic regulation alone.
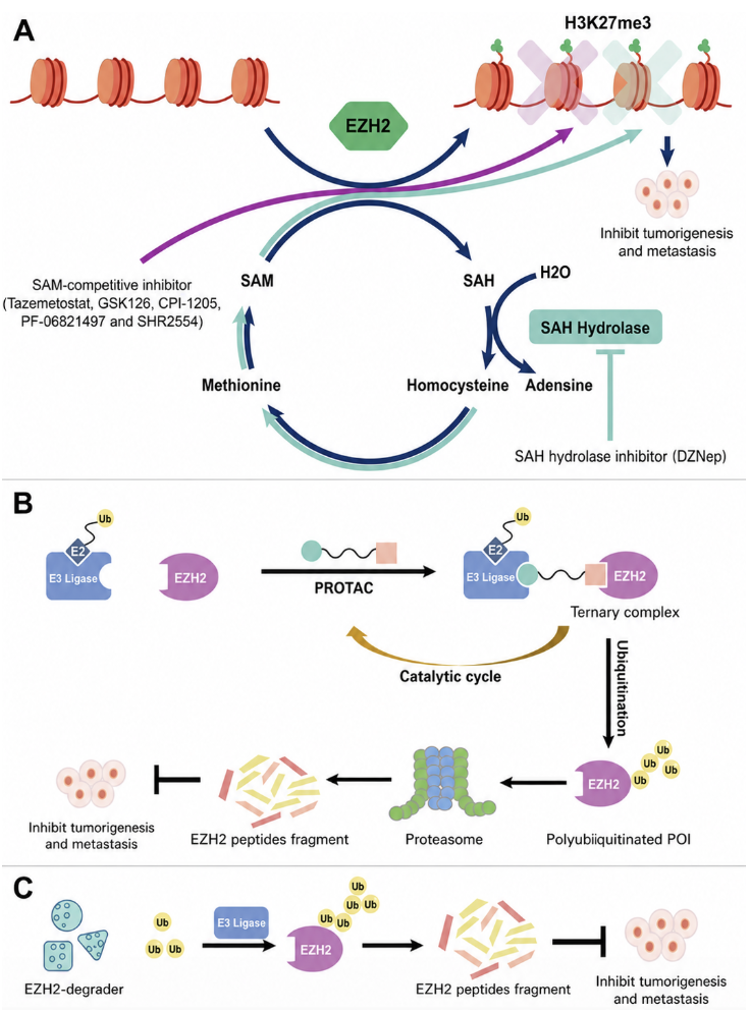
Figure 1: Therapeutic Strategies for Targeting EZH21
Preclinical studies have demonstrated that EZH2 overexpression is associated with aggressive disease biology, poor clinical outcomes, and resistance to AR-directed therapies. Mechanistically, EZH2 contributes to prostate cancer progression through transcriptional repression of tumor suppressor genes, activation of androgen receptor signaling programs, co-regulation of AR-mediated transcription, promotion of cell-cycle deregulation, and facilitation of lineage plasticity and neuroendocrine trans-differentiation. These findings have positioned EZH2 as an attractive therapeutic target, particularly in the setting of resistance to ARPI therapy.
Importantly, accumulating evidence suggests substantial biologic crosstalk between EZH2 and AR signaling pathways. As a result, inhibition of EZH2 may enhance the activity of AR-directed therapies, delay the development of resistance, and potentially restore sensitivity to hormonal treatment.
Mevrometostat: A Selective EZH2 Inhibitor Designed to Extend ARPI Benefit
Mevrometostat (PF-06821497) is an oral, potent, selective EZH2 inhibitor designed to target the epigenetic mechanisms contributing to prostate cancer progression and treatment resistance. Unlike ARPIs, which directly inhibit androgen receptor signaling, mevrometostat targets an upstream resistance pathway that appears to support continued AR activity despite hormonal therapy.
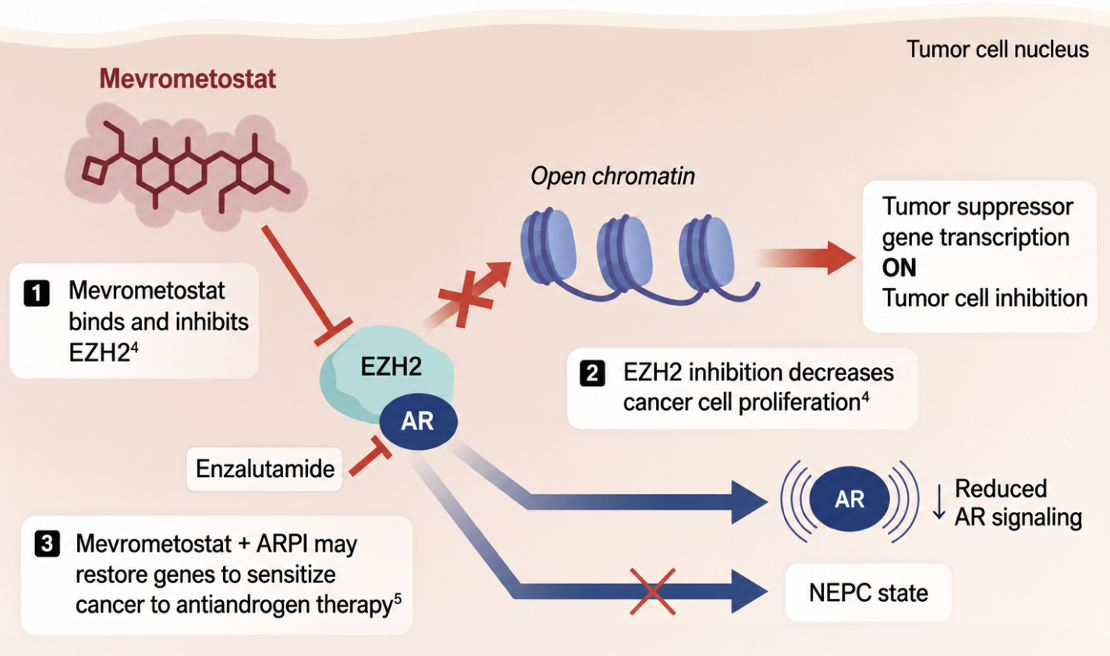
Figure 2: Proposed mechanism of mevrometostat
The rationale for combining mevrometostat with enzalutamide is based on the hypothesis that dual targeting of AR signaling and EZH2-mediated resistance mechanisms may prolong treatment response and delay disease progression. Early clinical evidence supporting this strategy emerged from the phase I/II study NCT03460977, which evaluated mevrometostat + enzalutamide in patients with heavily pretreated mCRPC. In this study, mevrometostat combined with enzalutamide demonstrated promising antitumor activity and a manageable safety profile. Among the most common adverse events considered related to mevrometostat were diarrhea, dysgeusia, and anemia. Notably, in a subgroup analysis presented at the 2026 ASCO GU annual meeting, patients treated with mevrometostat + enzalutamide achieved a median radiographic progression free survival of 14.3 months (95% CI 7.5, not estimable) compared with 6.2 months (95% CI 4.1, 13.9) for enzalutamide alone (HR 0.51, 90% CI 0.28–0.95) [2]. These findings provided the foundation for the phase III MEVPRO program.
MEVPRO-1: Targeting Post-Abiraterone mCRPC
MEVPRO-1 (NCT06551324) represents the first phase III evaluation of mevrometostat in patients with mCRPC who have progressed following treatment with abiraterone acetate.
The rationale for this study stems from a common clinical challenge encountered in contemporary practice: following progression on first-line abiraterone, many patients are transitioned to enzalutamide, particularly when chemotherapy is not desirable or feasible. However, cross-resistance between ARPIs often limits the efficacy of sequential hormonal therapy. By incorporating EZH2 inhibition, investigators aim to overcome resistance mechanisms and extend the clinical benefit of enzalutamide.
MEVPRO-1 is a global, open-label, randomized phase III study enrolling 600 patients with mCRPC. Eligible patients must be at least 18 years old, have radiographic progression following at least 12 weeks of abiraterone treatment, maintain castration-level testosterone concentrations ≤50 ng/dL, have an ECOG performance status of 0–2, and an anticipated life expectancy of at least six months. Participants are randomized 1:1 to receive either mevrometostat 875 mg orally twice daily with food + enzalutamide 160 mg daily or physician’s choice therapy consisting of enzalutamide monotherapy or docetaxel 75 mg/m² administered intravenously every 21 days. Randomization is stratified according to prior docetaxel exposure in the metastatic castration-sensitive setting, physician’s choice comparator arm, and the presence of hepatic metastases.
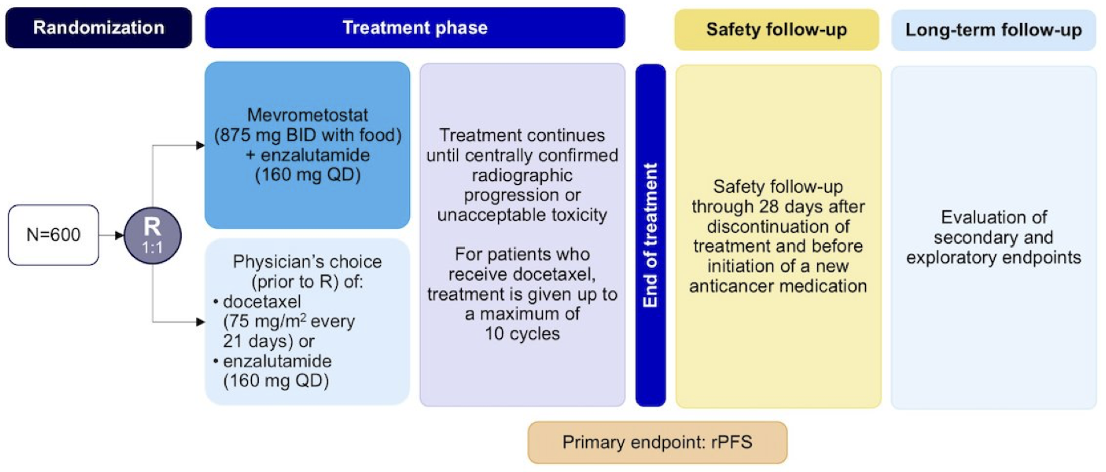
Figure 3: Study design for MEVPRO-1
The primary endpoint is radiographic progression free survival assessed by blinded independent central review using RECIST 1.1 criteria for soft tissue disease and PCWG3 criteria for bone metastases. Secondary endpoints include overall survival and additional efficacy, safety, and patient-reported outcome measures.
The first patient was enrolled on October 21, 2024. Enrollment is ongoing across Asia Pacific, Europe, Latin America, North America, and South Africa. Study completion is anticipated in October 2028. From a clinical perspective, MEVPRO-1 addresses an important therapeutic gap in post-abiraterone mCRPC and may establish a novel strategy for extending the utility of AR-directed therapy before transitioning patients to chemotherapy.
MEVPRO-2: Moving Earlier into ARPI-Naïve mCRPC
Whereas MEVPRO-1 focuses on patients after abiraterone exposure, MEVPRO-2 (NCT06629779) evaluates whether the addition of mevrometostat can enhance outcomes in patients with ARPI-naïve mCRPC. Rather than attempting to overcome established resistance, MEVPRO-2 seeks to delay or prevent the emergence of resistance altogether through simultaneous inhibition of EZH2 and AR signaling pathways.
MEVPRO-2 is a global, randomized, double-blind, placebo-controlled phase III study enrolling 900 patients with ARPI-naïve mCRPC. Patients are randomized 1:1 to receive either mevrometostat 875 mg twice daily + enzalutamide 160 mg daily or placebo + enzalutamide. Randomization is stratified according to prior docetaxel exposure in the metastatic CSPC setting and the presence of hepatic metastases. Unlike the open-label design employed in MEVPRO-1, MEVPRO-2 utilizes a placebo-controlled double-blind design, minimizing bias and providing a rigorous assessment of treatment effect.
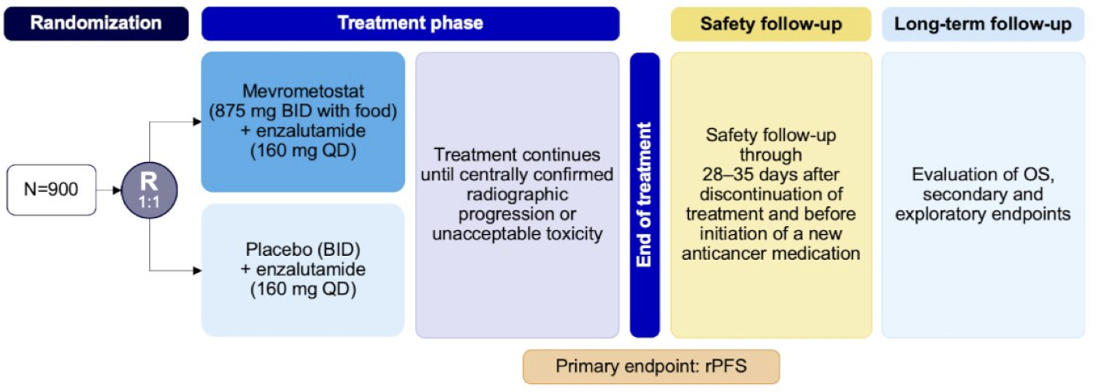
Figure 4: Study design for MEVPRO-2
The primary endpoint is radiographic progression free survival according to RECIST 1.1 and PCWG3 criteria, assessed by blinded independent central review. Key secondary endpoints include overall survival and time to pain progression. Additional secondary endpoints encompass objective response rate, duration of response, patient-reported outcomes, pharmacokinetics, and circulating tumor DNA burden.
The first patient was enrolled on October 22, 2024. Enrollment is ongoing across Asia Pacific, Europe, Latin America, North America, and South Africa, with study completion projected for November 2028. MEVPRO-2 is in a particularly important position within the advanced prostate cancer treatment landscape. If positive, the study could establish EZH2 inhibition as a strategy to prolong the effectiveness of first-line AR-directed therapy in mCRPC before resistance develops.
MEVPRO-3: Extending EZH2 Inhibition into mCSPC
The most ambitious component of the development program is MEVPRO-3 (NCT07028853), which moves EZH2 inhibition into the mCSPC setting. The rationale reflects a broader trend in prostate cancer drug development, where therapies initially developed in mCRPC are increasingly being evaluated earlier in the disease course. Given the activity observed with mevrometostat + enzalutamide in mCRPC, investigators hypothesize that introducing EZH2 inhibition during hormone sensitive disease space may delay progression to castration resistance and ultimately improve long-term survival outcomes.
MEVPRO-3 is a global, randomized, double-blind phase III study enrolling 1,000 patients with ARPI-naïve mCSPC. Eligible patients must be at least 18 years old and have an ECOG performance status of 0–1. Prior systemic therapy for metastatic disease is generally prohibited except for up to three months of ADT, with or without first-generation antiandrogens, provided there is no evidence of disease progression before study entry. Prior palliative radiotherapy or surgery is permitted, whereas prior radical prostatectomy, definitive prostate radiotherapy, and metastasis-directed therapy for mCSPC are not allowed.
Patients are randomized 1:1 to receive either mevrometostat 875 mg twice daily + enzalutamide 160 mg daily or placebo + enzalutamide. Randomization is stratified according to disease volume (low versus high) and disease presentation (de novo versus relapsed mCSPC).
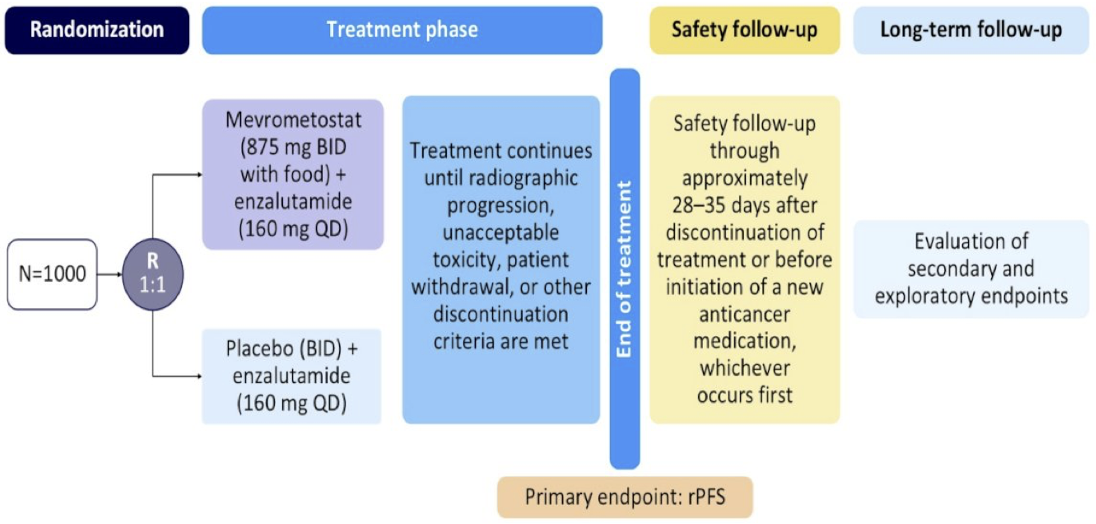
Figure 5: Study design for MEVPRO-3
The primary endpoint is radiographic progression free survival assessed by blinded independent central review using RECIST 1.1 and PCWG3 criteria. Secondary endpoints include overall survival, objective response rate, duration of response, time to PSA progression, initiation of new antineoplastic therapy, first symptomatic skeletal event, time to CRPC, patient reported outcomes, pharmacokinetics, and safety.
The first patient was enrolled on September 28, 2025. Enrollment is ongoing in North America and Asia-Pacific regions, with planned expansion into Europe and Latin America. Study completion is expected in December 2034. MEVPRO-3 represents the earliest disease setting currently being evaluated and reflects the hypothesis that targeting resistance mechanisms before they emerge may yield the greatest clinical benefit.
Potential Future Role of Mevrometostat in the Advanced Prostate Cancer Treatment Algorithm
Collectively, the MEVPRO clinical trial program represents a comprehensive strategy to evaluate EZH2 inhibition across multiple stages of advanced prostate cancer. Importantly, the three studies are positioned to answer complementary clinical questions:
- MEVPRO-1 investigates whether mevrometostat can overcome established resistance following abiraterone exposure
- MEVPRO-2 evaluates whether resistance can be delayed in ARPI-naïve mCRPC
- MEVPRO-3 seeks to determine whether the development of castration resistance itself can be postponed through earlier intervention in mCSPC
Perhaps most importantly, the MEVPRO program represents a shift beyond targeting androgen receptor signaling alone. By addressing the epigenetic mechanisms that contribute to resistance, mevrometostat has the potential to complement existing AR-directed therapies and extend their clinical benefit. Whether this approach ultimately changes the treatment paradigm will depend on the outcomes of the ongoing phase III studies. Nevertheless, the breadth of the MEVPRO clinical trial program underscores growing interest in EZH2 inhibition as a novel therapeutic strategy in advanced prostate cancer and may provide important insights into how resistance pathways can be targeted across the prostate cancer continuum.
Overview of the Phase III MEVPRO Clinical Development Program Evaluating Mevrometostat in Advanced Prostate Cancer
|
Characteristic |
MEVPRO-1 (NCT06551324) |
MEVPRO-2 (NCT06629779) |
MEVPRO-3 (NCT07028853) |
|
Disease Setting |
mCRPC |
mCRPC |
mCSPC |
|
Patient Population |
Post-abiraterone mCRPC with radiographic progression following ≥12 weeks of abiraterone treatment |
ARPI-naïve mCRPC |
ARPI-naïve mCSPC |
|
Study Design |
Global, randomized, open-label, phase III trial |
Global, randomized, double-blind, placebo-controlled phase III trial |
Global, randomized, double-blind, placebo-controlled phase III trial |
|
Intervention Arm |
Mevrometostat 875 mg orally twice daily with food + enzalutamide 160 mg daily |
Mevrometostat 875 mg orally twice daily with food + enzalutamide 160 mg daily |
Mevrometostat 875 mg orally twice daily with food + enzalutamide 160 mg daily |
|
Control Arm |
Physician’s choice of enzalutamide 160 mg daily or docetaxel 75 mg/m² IV every 21 days |
Placebo twice daily + enzalutamide 160 mg daily |
Placebo twice daily + enzalutamide 160 mg daily |
|
Goal Accrual |
600 patients |
900 patients |
1,000 patients |
|
Key Eligibility Criteria |
· Age ≥18 years · Radiographic progression following ≥12 weeks of abiraterone · Testosterone ≤50 ng/dL · ECOG 0–2 · Life expectancy ≥6 months |
· Age ≥18 years · ARPI-naïve mCRPC · Protocol-defined eligibility criteria · Prior docetaxel for mCSPC permitted |
· Age ≥18 years · mCSPC · ECOG 0–1 · ≤3 months prior ADT (with or without first-generation antiandrogens) · No prior progression before study entry |
|
Randomization Stratification Factors |
· Prior docetaxel use in mCSPC · Physician’s choice comparator (enzalutamide versus docetaxel) · Presence of hepatic metastases |
· Prior docetaxel use in mCSPC · Presence of hepatic metastases |
· Disease volume (high versus low) · de novo versus relapsed mCSPC |
|
Primary Endpoint |
rPFS by blinded independent central review using RECIST 1.1 and PCWG3 criteria |
rPFS by blinded independent central review using RECIST 1.1 and PCWG3 criteria |
rPFS by blinded independent central review using RECIST 1.1 and PCWG3 criteria |
|
Key Secondary Endpoints |
· OS and additional efficacy · Safety · PROs |
· OS · TT pain progression · ORR · DoR · PROs · Pharmacokinetics · ct DNA burden |
· OS · ORR · DoR · TT PSA progression · Initiation of new antineoplastic therapy · First SSE · TT CRPC · PROs · Pharmacokinetics · Safety |
|
Recruiting Regions |
Asia Pacific, Europe, Latin America, North America, and South Africa |
Asia Pacific, Europe, Latin America, North America, and South Africa |
North America and Asia-Pacific currently active; Europe and Latin America planned |
|
Estimated Study Completion |
October 2028 |
November 2028 |
December 2034 |
|
Potential Clinical Impact if Positive |
Could establish mevrometostat + enzalutamide as a post-abiraterone treatment strategy and alternative to immediate chemotherapy escalation |
Could support incorporation of EZH2 inhibition alongside first-line ARPI therapy in mCRPC |
Could move EZH2 inhibition into frontline mCSPC treatment intensification and potentially reshape the metastatic disease treatment algorithm |
Written by: Zachary Klaassen, MD, MSc, Urologic Oncologist, Wellstar MCG Health, Augusta, Georgia, USA
References:
- Guo Y, Cheng R, Wang Y, et al. Regulation of EZH2 protein stability: New mechanisms, roles in tumorigenesis, and roads to the clinic. eBioMedicine 2024;100:104972.
- Matsubara N, Gordoa TA, Moreno A, et al. Efficacy and safety of mevrometostat in combination with enzalutamide in patients with mCRPC: Data from a phase 1 study. J Clin Oncol. 2026;44(195):Suppl_195.