(UroToday.com) In the session of the 2022 Advanced Prostate Cancer Consensus Conference focusing on the treatment of patients with metastatic castration-resistant prostate cancer (mCRPC), Dr. Matthew Smith discussed the role of prostate specific membrane antigen (PSMA)-lutetium radionuclide therapy, including considerations regarding monotherapy, combination therapy, and patient selection.
He first highlighted that PSMA is a transmembrane carboxypeptidase that is highly expressed in prostate cancer but has relatively low expression in normal tissues. As a result, PSMA has been utilized as a target for PET imaging, radioligand therapy, and adoptive cellular therapy. In the context of radioligand therapy, he highlighted that the VISION trials have, in a phase III fashion, shown this to be a validated target in mCRPC. Notably, this study of lutetium-PSMA radioligand therapy required evidence of 68Ga-PSMA uptake without evidence of PSMA negative tumor sites.
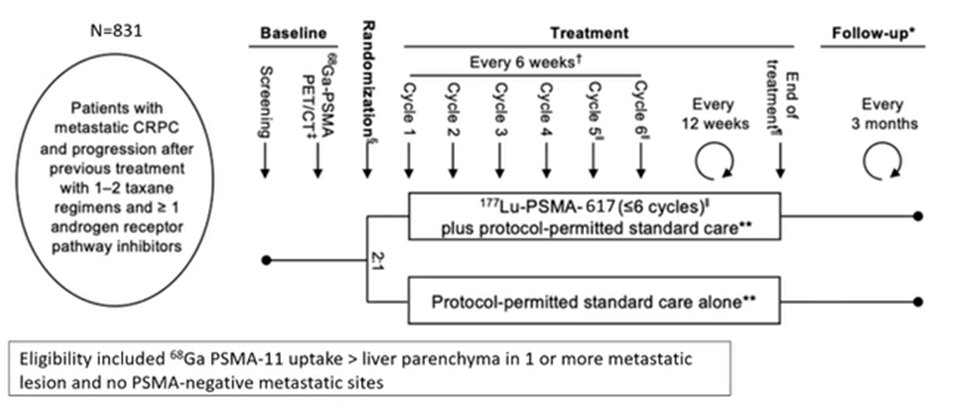
In describing the results of VISION, Dr. Smith referred to this as a “spectacularly positively trial” with evidence of a statistically significant 5.3 month improvement in radiographic progression-free survival and 4 month improvement in overall survival. He further noted that while subgroup analysis showed generally consistent results, there was a somewhat greater improvement among those patients who received androgen receptor pathways inhibitors as part of their planned standard of care. While there are a number of potential explanations for this finding, including chance or unintended bias, this may represent increased target expression based on the combination of therapies. There are a number of ongoing trials of combination approaches which include Lutetium-PSMA radioligand therapy that will explore this in a more fulsome manner.
Dr. Smith then moved on to discuss the TheraP trial which, in a phase II fashion, assessed the role of lutetium-PSMA radioligand therapy, compared to cabazitaxel, in patients with prior docetaxel and novel hormonal therapy. Notably, the selection approach here was somewhat different with an SUVmax of 20 or greater required at an index lesion, with other metastatic sites having SUVmax of 10 or more on PSMA-PET/CT. Patients further underwent FDG-PET/CT and those with discordant disease were excluded. While the overall results of TheraP demonstrated that PSA responses were significantly more common in patients receiving lutetium-PSMA therapy, he particularly emphasized that this was seen independent of baseline PSMA intensity. However, there was evidence of effect modification with a significantly larger difference between lutetium-PSMA and cabazitaxel seen among patients with higher PSMA SUVmax (>10), than those with lower levels. Thus, he suggested that these “marked differences” shows that baseline intensity may be a predictive biomarker.

While VISION established lutetium-PSMA radioligand therapy as a new standard of care among patients with very advanced disease, there is now a “wave of new trials” assessing both monotherapy and combination therapy approaches across a variety of prostate cancer disease spaces. Compared to other combination trials, he suggested that many of these trials have a particularly “rationale” design and approach.
Moving forward, while VISION established lutetium-PSMA radioligand therapy as a new standard of care and led to FDA approval, there are many gray areas that result from this study, particularly as it relates to FDA approval. First, the trial utilized (and the FDA approval mandates) patient identification and selection using 68Ga-PSMA-11 imaging. However, other approaches (including 18F-DCFPyL, rhPSMA, and others) are increasingly utilized. Further, while all patients in VISION had previously received cytotoxic chemotherapy, what is the role of this treatment in patients who are unfit for docetaxel? Finally, among patients who initially respond, is there a role for re-treatment?
Thus, in conclusion, he emphasized that 177Lu-PSMA-617 is now a treatment option for patients with heavily pretreated mCRPC with evidence of significantly improved survival. Baseline PSMA avidity appears to be predictive of the response to treatment and may help guide patient selection. Numerous outstanding questions will be addressed in ongoing and planned studies.
Presented by: Matthew Smith, MD, PhD, Claire and John Bertucci Endowed Chair in Genitourinary Cancers, Professor of Medicine, Harvard Medical School