The landscape for metastatic castration resistance prostate cancer continues to rapidly change. Therapies move forward from CRPC to castration-sensitive prostate cancer. There have been novel targeted drugs for metastatic castration resistance prostate cancer. There’s also new data on the treatment sequence in this disease space.
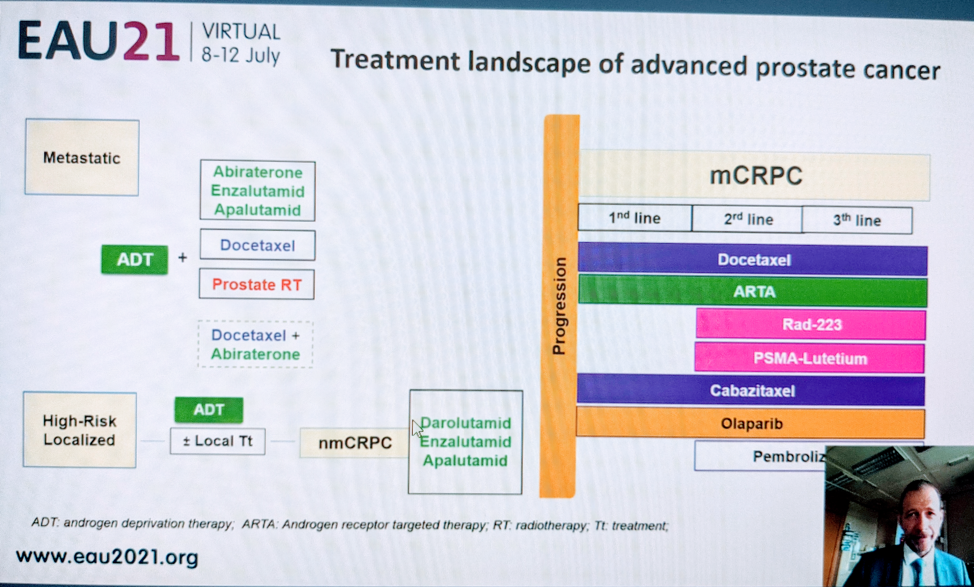
He shared a slide on the treatment landscape as it stands now.
Two new phase 3 trials that have been published are worth discussing in further detail. The PROFOUND1 study and the VISION2 study.
The PROFOUND study was previously presented and the full discussion can be found here. It is the first randomized phase III study evaluating a PARP-inhibitor vs. new hormonal agents in patients with HRR mutations and mCRPC.
The study design is below:
The study met its primary endpoint – olaparib significantly improved rPFS in patients with alterations in BRCA1, BRCA2, and ATM mutations vs. physician's choice (HR 0.34 (95% confidence interval 0.25 to 0.47)). It was generally well tolerated.
The second study was the VISION study, presented earlier this year at ASCO.
Lutetium bound PSMA is used to target prostate cancer. One of the approaches gaining the most interest is so-called “theranostics” – in prostate cancer, this approach leverages molecularly targeting cancer cells using prostate-specific membrane antigen (PSMA)-targeting radioligands. As PSMA is highly expressed in prostate cancer and mCRPC lesions, the combination of PSMA-617 with the beta-emitter lutetium allows for the targeted delivery of ß-particle radiation to PSMA-expressing cells and the surrounding microenvironment.
The study design is below:
Over a median study follow-up of 20.9 months (as of a data cut-off of 27 January 2021), treatment with 177Lu-PSMA-617 + SOC significantly improved overall survival by a median of 4.0 months (median overall survival (OS), 15.3 vs 11.3 months; HR, 0.62 [95% CI: 0.52, 0.74]; p < 0.001, one-sided), compared to SOC alone, in the overall cohort of all randomized patients (n=831).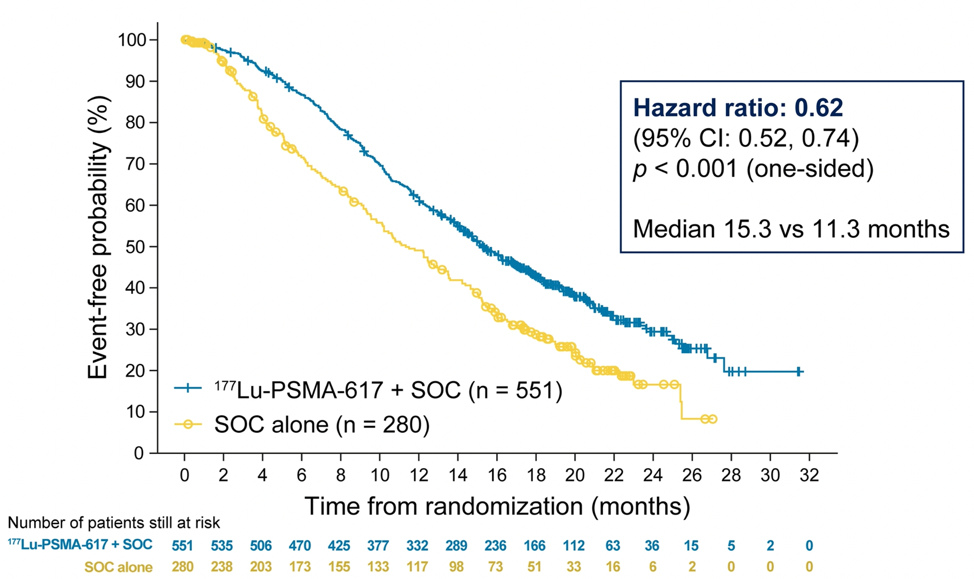
Importantly, it also demonstrated an impressive objective response rate – with 9% (vs. 0% of controls) have a complete response and 41.8% (vs. 3.1% of controls) have a partial response.
The safety profile was also tolerable. While a higher rate of high-grade (grade 3-5) treatment-emergent adverse events was observed with 177Lu-PSMA-617 (28.4% vs 3.9%), overall therapy was well tolerated. However, it bears note that there were 5 deaths attributable to 177Lu-PSMA-617 treatment. In terms of specific adverse events, treatment with 177Lu-PSMA-617 + SOC was associated with increased rates of bone marrow suppression, xerostomia, and nausea and vomiting.
In terms of sequencing of therapies, he did briefly touch on the CARD trial.3 This was a study to assess whether you could rechallenge a patient with an AR targeted agent in mCRPC setting – compared against cabazitaxel.
The study design is below: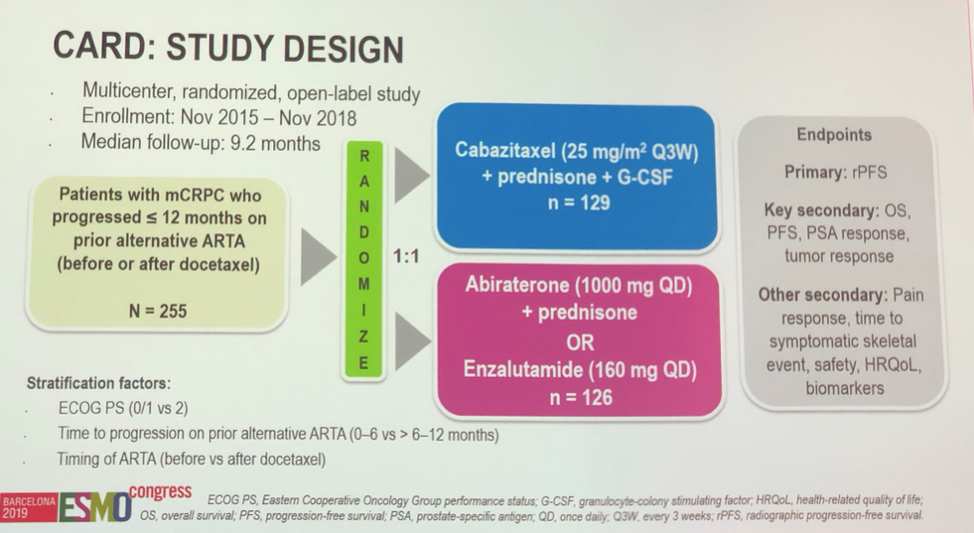
Ultimately, this study demonstrated that radiographic PFS and OS both favored cabazitaxel over alternative AR targeted agents. Hence, it does not look like rechallenge with AR targeted agents makes sense.
His take home messages from the talk are:
1. Novel targeted therapies, such as olaparib and Lutetium-PSMA – are being introduced
2. There is a need for genetic testing in molecular imaging
3. Do not give an AR targeted agent after AR targete therapy due to cross resistance
4. Monitoring for AR targeted agent side effects and bone health are necessary
5. There’s an urgent need for head-to-head studies
Presented by: Gero Kramer, MD, Urologist, the Medical University of Vienna
Written by: Thenappan (Thenu) Chandrasekar, MD – Urologic Oncologist, Assistant Professor of Urology, Sidney Kimmel Cancer Center, Thomas Jefferson University, @tchandra_uromd on Twitter during the 2021 European Association of Urology, EAU 2021- Virtual Meeting, July 8-12, 2021.
References:
1. Hussain M, Mateo J, Fizazi K, et al. Survival with Olaparib in Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2020 Dec 10;383(24):2345-2357. doi: 10.1056/NEJMoa2022485. Epub 2020 Sep 20. PMID: 32955174.
2. Sartor O, de Bono J, Chi KN, et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Jun 23. doi: 10.1056/NEJMoa2107322. Epub ahead of print. PMID: 34161051.
3. de Wit R, de Bono J, Sternberg CN, et al. Cabazitaxel versus Abiraterone or Enzalutamide in Metastatic Prostate Cancer. N Engl J Med. 2019 Dec 26;381(26):2506-2518. doi: 10.1056/NEJMoa1911206. Epub 2019 Sep 30. PMID: 31566937.