Barcelona, Spain (UroToday.com) Despite significant progress in systematic therapy, metastatic castration-resistant prostate cancer (mCRPC) continues to be a lethal disease. mCRPC is molecularly heterogeneous, as up to 30% of mCRPC harbor deleterious alterations in DNA damage repair genes, including those with direct and indirect roles in homologous recombination repair. These loss-of-function alterations in homologous recombination repair genes are associated with response to PARP inhibition, of which BRCA1, BRCA2, and ATM are the most well characterized.
Furthermore, anti-tumor activity has been reported with the PARP inhibitor olaparib in patients with prostate cancer harboring homologous recombination repair alterations. PROfound was a randomized, open-label, phase III trial evaluating efficacy and safety of olaparib vs enzalutamide or abiraterone in patients with mCRPC with alterations in any of 15 predefined genes with a direct or indirect role in homologous recombination repair whose disease had progressed on prior new hormonal agent therapy. At the Presidential session at ESMO 2019, Maha Hussain, MD, and colleagues presented the initial results of PROfound.
For PROfound, qualifying tumour tissue homologous recombination repair alterations were centrally and prospectively identified using an investigational next-generation sequencing test. Cohort A included patients with alterations in BRCA1, BRCA2 or ATM, while Cohort B patients included any one of 12 other homologous recombination repair alterations (BRIP1, BARD1, CDK12, CHEK1, CHEK2, FANCL, PALB2, PPP2R2A, RAD51B, RAD51C, RAD51D or RAD54L). Patients were randomized 2:1 to olaparib (300 mg bid) or the physician’s choice of enzalutamide (160 mg/day) or abiraterone (1000 mg/day + prednisone 5 mg BID). The primary endpoint was radiographic progression-free survival (rPFS) in Cohort A, assessed by blinded independent central review and analyzed via a stratified log-rank test. Crossover to olaparib was allowed after blinded independent central review progression.
Trial design for PROfound: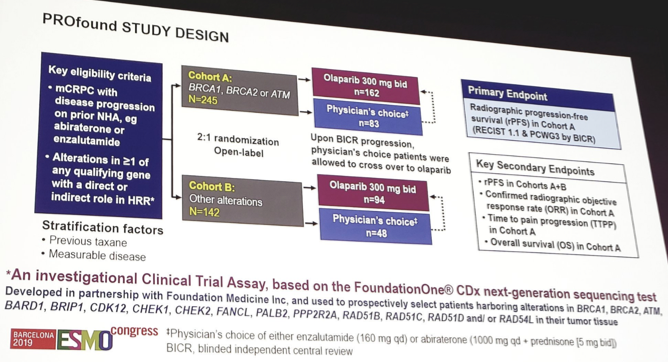
The target sample size was 240 subjects for Cohort A, with a target hazard ratio of 0.53 with 95% power and 2-sided 5% alpha (143 events). A hierarchical testing design was instituted whereby if the primary endpoint demonstrated statistical significance, the key secondary endpoints were tested sequentially. Patients were randomized between April 2017 and November 2018, with a data cutoff of June 4, 2019.
There were 4,425 men screened for PROfound, leading to 245 randomized to Cohort A, and 142 to Cohort B (of which 65.6% had prior taxane chemotherapy). The median treatment duration was 7.4 months for olaparib and 3.9 months for enzalutamide/abiraterone. Olaparib was associated with improved rPFS compared to enzalutamide/abiraterone among patients in Cohort A (HR 0.34, 95% CI 0.25-0.47), which was consistent across the majority of subgroups assessed. 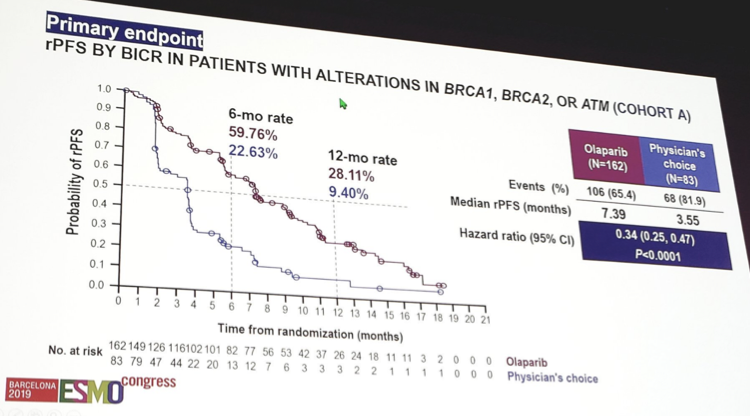
Furthermore, patients in Cohort A had a confirmed ORR of 33.3% for olaparib compared to 2.3% for enzalutamide/abiraterone (OR 20.86, 95% CI 4.18-379.18). A key secondary endpoint was time to pain progression in Cohort A, which also favored olaparib (HR 0.44, 95% CI 0.22-0.91).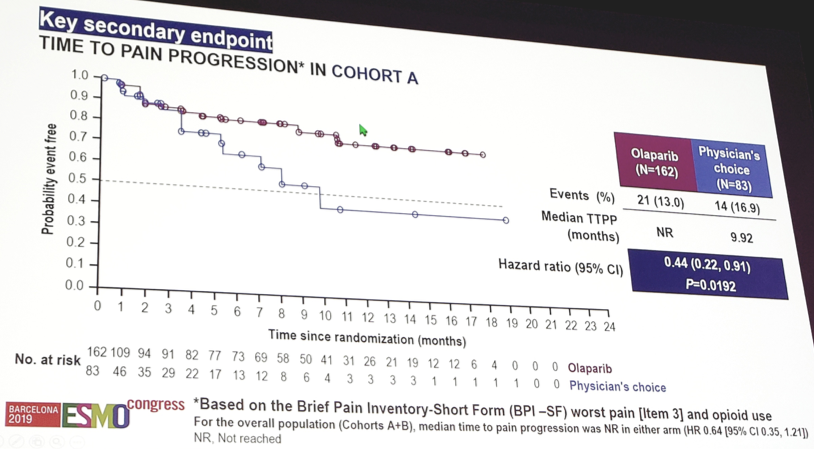
rPFS by blinded independent central review in the overall cohort, also favored olaparib (HR 0.49, 95% CI 0.38-0.63). The interim results for overall survival (OS) demonstrated improved survival among patients in Cohort A (HR 0.64, 95% CI 0.43-0.97), as well as for Cohort A+B (HR 0.67, 95% CI 0.49-0.93). 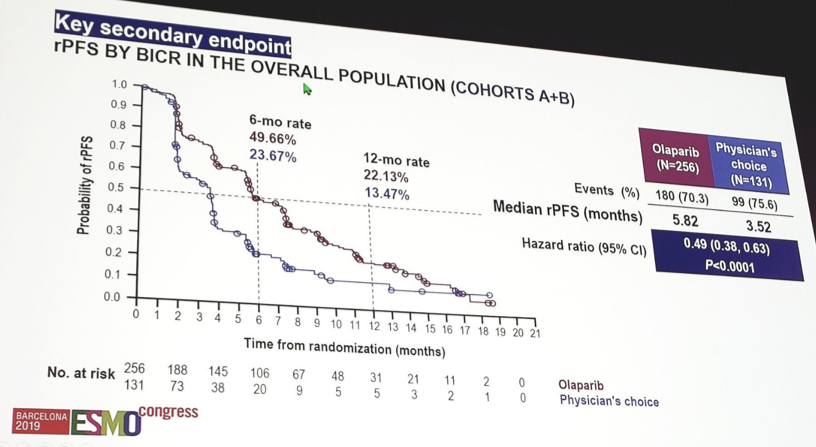
Of note, for the patients in the physician’s choice of enzalutamide/abiraterone arm who progressed, 80.6% in Cohort A and 84.6% in Cohort B crossed over to receive olaparib. When looking specifically at the Cohort B patients, there was no advantage to olaparib in the rPFS by blinded independent central review (HR 0.88, 95% CI 0.58-1.36) or in OS (HR 0.73, 95% CI 0.45-1.23), however there was a benefit to olaparib for rPFS by investigator assessment (HR 0.60, 95% CI 0.39-0.93).
The most common adverse events were anemia (46.1% vs 15.4%), nausea (41.4% vs 19.2%), decreased appetite (30.1% vs 17.7%) and fatigue (26.2% vs 20.8%) for olaparib vs enzalutamide/abiraterone. Among patients receiving olaparib, 16.4% discontinued treatment secondary to an adverse event, compared to 8.5% of patients receiving enzalutamide/abiraterone. Interestingly, 4.3% of patients receiving olaparib had a pulmonary embolism, compared to 0.8% among those receiving enzalutamide/abiraterone, none of which were fatal. There were no reports of myelodysplastic syndrome or acute myeloid leukemia.
In an exploratory analysis of gene-by-gene rPFS, 7/15 genes had alteration frequencies too low for descriptive statistics, however 97% of patients were randomized based on alterations in 8/15 single genes. Of note, there is evidence of clinical activity of olaparib in patients with alterations in genes other than BRCA1 and BRCA2. However, gene-level analysis is complex and exploratory, and comparisons may be confounded by multiple factors.
Dr. Hussain concluded her presentation of PROfound with several key conclusions:
- In patients with mCRPC and homologous recombination repair alterations with prior treatment, olaparib improved rPFS and ORR compared to enzalutamide/abiraterone, with a favorable trend for OS despite crossover. This was specifically noted in patients with BRCA1, BRCA2 and ATM mutations.
- Safety was generally consistent with the known profile of olaparib.
- PROfound is the first positive phase III biomarker-selected study evaluating a molecularly targeted treatment in patients with mCRPC, which highlights the importance of genomic testing in this population.
Presented by: Maha Hussain, MD, Professor of Medicine and Deputy Director of the Robert H. Lurie Comprehensive Cancer Center of Northwestern University, Chicago, IL
Co-Authors: J. Mateo 2, K. Fizazi 3, F. Saad 4, N. Shore 5, S. Sandhu 6, K. Chi 7, O. Sartor 8, N. Agarwal 9, D. Olmos 10, A. Thiery-Vuillemin 11, P. Twardowski 12, N. Mehra 13, C. Goessl 14, J. Kang 14, J. Burgents 15, W. Wu 14, A. Kohlmann 16, C. Adelman 17, J. De Bono 18
2. Vall d'Hebron University Hospital, Barcelona, ES
3. Institut Gustave Roussy, Villejuif, FR
4. Centre Hospitalier de l’Université de Montréal/CRCHUM, Montreal, CA
5. Carolina Urologic Research Center, Myrtle Beach, US
6. Peter MacCallum Cancer Centre, Melbourne, AU
7. BC Cancer Agency - Vancouver, Vancouver, CA
8. Tulane University School of Medicine, New Orleans, US
9. Huntsman Cancer Institute, Salt Lake City, US
10. Spanish National Cancer Research Centre (CNIO), & Hospitales Universitarios Virgen de la Victoria y Regional de Málaga, Madrid, ES
11. CHRU Besancon - Hospital Jean Minjoz, Besançon, FR
12. City of Hope, Duarte, US
13. Radboud University Medical Center, Nijmegen, NL
14. AstraZeneca, Gaithersburg, US
15. Merck, Sharpe & Dohme NA, Kenilworth, US
16. AstraZeneca UK, Royston, UK
17. AstraZeneca, Cambridge, UK
18. The Institute of Cancer Research and Royal Marsden, London, UK
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md at the 2019 European Society for Medical Oncology annual meeting, ESMO 2019 #ESMO19, 27 Sept - 1 Oct 2019 in Barcelona, Spain
Further Related Content:
Read: Olaparib Regulatory Submission Granted Priority Review in the US for HRR-Mutated Metastatic Castration-Resistant Prostate Cancer
Watch: PROfound Study - PARP-inhibitor Olaparib in Advanced Prostate Cancer Patients with Specific Tumor Mutations - Maha Hussain