To address this question, we conducted a multicenter retrospective study including 487 patients treated across eight French academic institutions between 2014 and 2023. Among them, 182 patients (37.4%) underwent robotic-assisted BCE (RA-BCE) and 305 (62.6%) underwent open BCE (O-BCE).
Oncological Outcomes
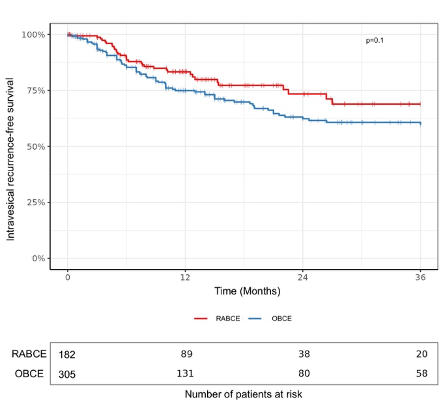
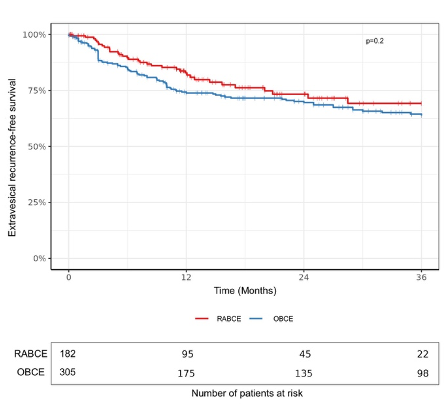
After a median follow-up of 30 months, intravesical recurrence occurred in 23.2% of patients, with a median time to recurrence of 7.5 months. Importantly, the 3-year intravesical recurrence-free survival was similar between RA-BCE and O-BCE (68.9% vs 59.7%, log-rank p=0.1). Robotic BCE was not independently associated with bladder recurrence on multivariable analysis (HR 0.77, p=0.2). Similarly, 3-year extravesical recurrence-free survival (69.2% vs 63.8%,log-rank p=0.2), cancer-specific survival, and overall survival were also comparable between the two approaches. These findings remained consistent in sensitivity analyses excluding patients with prior bladder cancer.
Perioperative Outcomes
Beyond oncologic safety, robotic BCE was associated with improved perioperative outcomes. Patients treated with RA-BCE experienced significantly fewer overall 90-day postoperative complications (10.1% vs 21.3%, p=0.02), fewer major complications (4.7% vs 7.1%, p=0.02), and shorter hospital stay (5 vs 7 days, p<0.01). Duration of bladder catheterization was similar between groups.
|
Outcomes |
Overall (n=340, 100%*) |
RA-BCE (n=129, 37.9%) |
O-BCE (n=211, 62.1%) |
p-value |
|
Perioperative |
||||
|
Median OR time, min (IQR) |
263 [220;330] |
256 [231; 312] |
265 [210;353] |
0.7 |
|
Median blood loss, ml (IQR) |
200 [100;400] |
175 [100; 300] |
200 [150; 400] |
0.8 |
|
Perioperative blood transfusion, n (%) |
36 (10.6) |
13 (10.1) |
23 (10.9) |
0.8 |
|
90-day complications, n (%) Absent Present Clavien-Dindo Grade ≤2 Clavien-Dindo Grade ≥3 |
282 (82.9) 58 (17.1) 37 (10.9) 21 (6.2) |
116 (89.9) 13 (10.1) 7 (5.4) 6 (4.7) |
166 (78.7) 45 (21.3) 30 (14.2) 15 (7.1) |
0.02 |
|
Median initial LoS, days [IQR] |
6 [5; 9] |
5 [4;6.25] |
7 [5;11] |
<0.01 |
|
Functional |
||||
|
Median bladder catheterization, days [IQR] |
5 [5;7] |
5 [4.25;7] |
6 [5;7] |
0.2 |
*340/487 patients evaluated.
Taken together, these findings suggest that robotic intracorporeal bladder cuff excision can achieve oncologic outcomes comparable to the open approach while preserving the perioperative benefits of minimally invasive surgery. Although prospective validation remains needed, our results support the growing role of fully robotic RNU in the management of localized UTUC.
Written by: Pierre-Etienne Gabriel,1 Thomas Seisen,2 Evanguelos Xylinas,3 Hugo Duquesne,4 Gautier Marcq,4 Igor Duquesne,5 Anne Sophie Bajeot,6 Jérémy Mercier,6 Benjamin Pradère,7 Louise Duffaut,8 Frederic Panthier,8 Yves Allory,9 François Audenet,10 Priscilla Leon,11 Constance Thibault,12 Morgan Rouprêt,2 Mathieu Roumiguié,13 Alexandra Masson-Lecomte,1
- Department of Urology, Université de Paris, APHP, Saint Louis Hospital, Paris, France.
- Sorbonne University, GRC 5 Predictive Onco-Uro, AP-HP, Urology, Hôpital Pitié-Salpetrière, Paris, France.
- Department of Urology, Bichat Claude-Bernard Hospital, Assistance Publique-Hôpitaux de Paris Nord, University Paris Cité, Paris, France.
- Urology Department, Claude Huriez Hospital, CHU Lille, University Lille, CNRS, CHU Lille, Institut Pasteur de Lille, UMR9020-U1277 - CANTHER - Cancer Heterogeneity Plasticity and Resistance to Therapies, Lille, Inserm, France.
- Department of Urology, Hôpital Cochin, AP-HP, Université de Paris, Paris, France.
- Urology Department, Toulouse University Hospital, University of Toulouse UT3, Toulouse, France.
- UROSUD Urology Department, Clinique Croix Du Sud, Quint-Fonsegrives, France.
- GRC n°20, Groupe de Recherche Clinique sur la Lithiase Urinaire, Hôpital Tenon, Sorbonne Université, Paris, France.
- Department of Pathology, Institut Curie, Université Paris Saclay, Saint-Cloud, France.
- Department of Urology, Hôpital Européen Georges-Pompidou AP-HP Centre, Université Paris Cité, Paris, France.
- Urology Department, Clinique Pasteur, Royan, France.
- Medical Oncology Department, Hôpital européen Georges-Pompidou AP-HP Centre, Université Paris Cité, Paris, France.
- Urology Department, Clinique Pasteur, Toulouse, France.