Upper tract urothelial carcinomas (UTUC) are considered an uncommon malignancy.1 Despite optimal treatment for the UTUC, metachronous bladder recurrences (M-NMIBC) can occur in 3-50% pr patients. Due to its rarity and the resultant lack of specific guidelines, patients with bladder recurrence following nephroureterectomy have historically been managed using treatment paradigms similar to those for primary bladder cancers (P-NMIBC), despite emerging evidence demonstrating inferior clinical outcomes compared to their lower tract counterparts.2-4
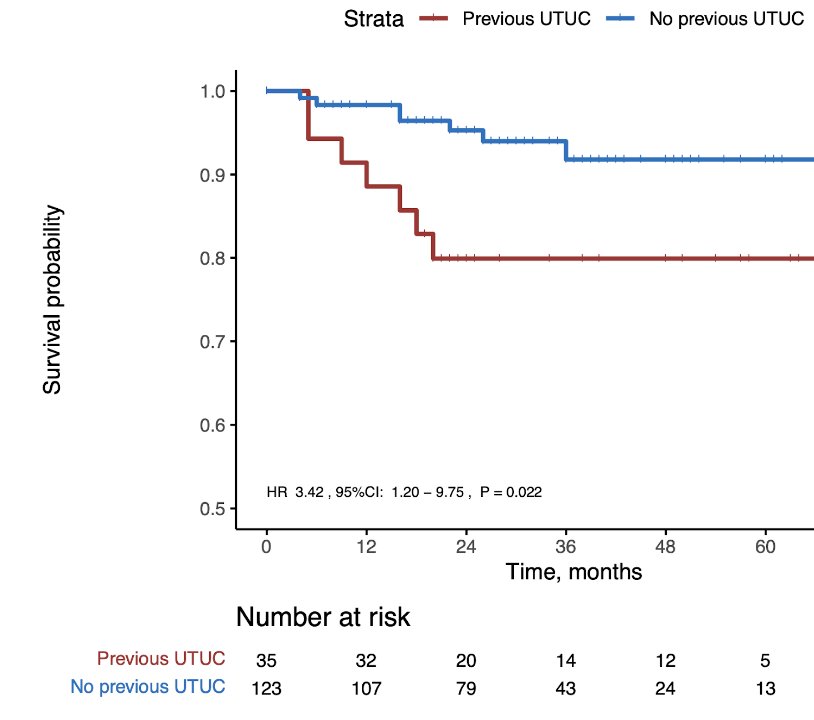
Our study offers a compelling insight into a clinically relevant but underexplored domain: the effectiveness of Bacillus Calmette-Guérin (BCG) therapy in high-grade non-muscle invasive bladder cancer (NMIBC) occurring after prior treatment for UTUC. Through a rigorously designed propensity-matched analysis, we demonstrated that patients with M-NMIBC had significantly higher rates of BCG failure, intravesical recurrence, and progression to muscle-invasive disease compared to those with P-NMIBC. Almost half with M-NMIBC will have high grade bladder recurrences after BCG, with a quarter progressing to muscle-invasive or metastatic disease. The alarmingly high rates of disease recurrence and progression suggest that prior UTUC is not merely a historical footnote in a patient’s oncological journey, but rather an active contributor to subsequent treatment resistance and tumour aggressiveness in the lower tract. This work reinforces the growing understanding that urothelial tumours arising in different locations, though histologically similar, are biologically distinct entities.5-6
(1A)

(1B)
(1C)
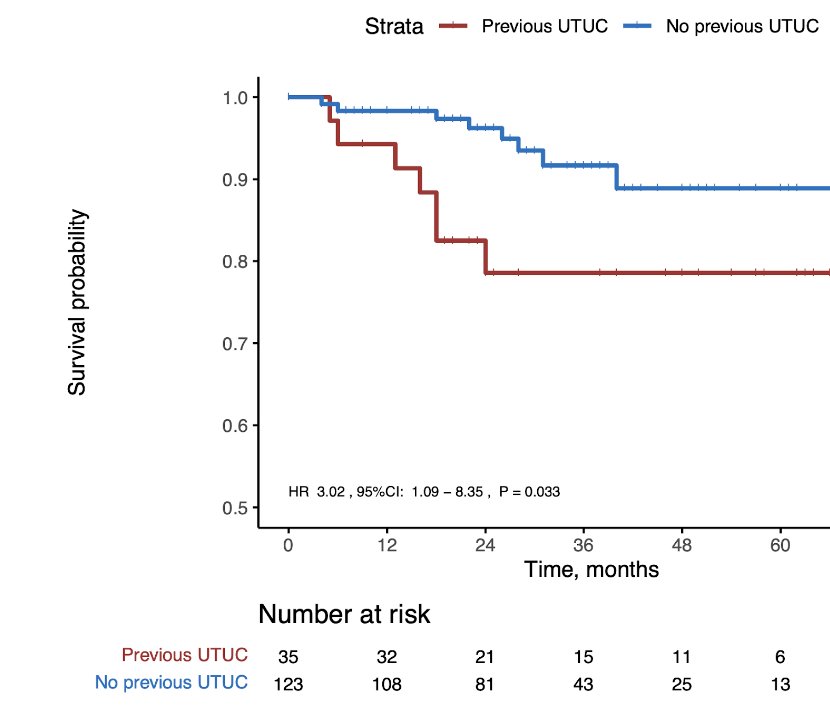
Our study’s most notable findings are the paradoxical observation that M-NMIBC tumours tend to be smaller and lower T staging, ostensibly because of early detection from routine surveillance cystoscopy, yet still had worse outcomes. This underscores the probable clonal relationship between UTUC and its subsequent metachronous bladder recurrences, supported by recent molecular studies identifying FGFR3 overexpression and immune-depleted tumour microenvironments in the M-NMIBC subgroup.7-8 These molecular differences likely compromise BCG’s immune-mediated mechanism of action, suggesting a need for personalized therapeutic strategies.9
Table 1: Clinicopathological characteristics of patients included in this study|
Before matching |
After propensity matching |
|||||
|
Variable |
M-NIMBC |
P-NMBIC |
P value |
P-NMBIC |
P value |
SMD |
|
Number of patients, n |
35 |
148 |
123 |
|||
|
Gender, n (%) |
0.697 |
0.555 |
0.153 |
|||
|
Men |
25 (71.4) |
113 (76.4) |
96 (78.0) |
|||
|
Female |
10 (28.6) |
35 (23.6) |
27 (22.0) |
|||
|
Age (mean (SD)) at NMIBC diagnosis |
75.00 (10.37) |
77.02 (9.82) |
0.280 |
77.01 (9.13) |
0.267 |
0.206 |
|
Smoker (%) |
0.542 |
0.701 |
0.161
|
|||
|
Active smoker |
6 (17.1) |
35 (23.6) |
27 (22.0) |
|||
|
Ex-Smoker |
11 (31.4) |
35 (23.6) |
31 (25.2) |
|||
|
Non-smoker |
18 (51.4) |
78 (52.7) |
65 (52.8) |
|||
|
Symptom present at diagnosis |
<0.001 |
<0.001 |
1.352 |
|||
|
Symptomatic |
8 (23.9) |
129 (79.7) |
97 (78.9) |
|||
|
Asymptomatic |
27 (77.1) |
30 (20.3) |
26 (21.1) |
|||
|
Number of tumors |
0.481 |
0.298 |
0.254 |
|||
|
1-2 |
29 |
100 |
89 |
|||
|
3 or more |
6 |
48 |
34 |
|||
|
Size of largest tumor (mm (mean (SD))) |
15.4 (9.6) |
25.7 (15.3) |
0.001 |
27.3 (15.5) |
<0.001 |
0.928
|
|
T staging on diagnosis |
<0.001 |
<0.001 |
0.605 |
|||
|
Ta |
17 (48.6) |
66 (44.6) |
59 (48.0) |
|||
|
T1 |
13 (37.1) |
82 (55.4) |
64 (52.0) |
|||
|
Isolated Cis |
5 (14.3) |
0 (0.0) |
0 (0.0) |
|||
|
CIS |
0.505 |
0.304 |
0.234 |
|||
|
Positive |
9 (25.7) |
28 (28.9) |
20 (16.3) |
|||
|
Negative |
26 (74.3) |
120 (81.1) |
103 (83.7) |
|||
|
EAU NMIBC risk stratification (%) |
0.284 |
0.567 |
0.200
|
|||
|
Intermediate Risk |
17 (48.6) |
33 (22.3) |
31 (25.2) |
|||
|
High risk |
13 (37.1) |
94 (63.5) |
80 (65.0) |
|||
|
Very high risk |
5 (14.3) |
21 (14.2) |
12 (9.8) |
|||
|
Presence of variant histo during TURBT |
0.118 |
0.075 |
0.468
|
|||
|
Yes |
1 (2.9) |
21 (14.2) |
20 (16.3) |
|||
|
No |
34 (97.1) |
127 (85.8) |
103 (83.7) |
|||
Clinically, these findings argue for a reassessment of standard BCG protocols in M-NMIBC patients and raise important questions regarding risk stratification. Should a history of UTUC prompt consideration of early radical treatment or alternate intravesical regimens? Should molecular profiling be routine in guiding therapy in such cases?
We hope to have shined a necessary spotlight on the unique clinical trajectory of M-NMIBC post-UTUC. Our findings not only challenge the one-size-fits-all paradigm of intravesical therapy but also support the integration of tumour biology into clinical decision-making. UTUC history should no longer be considered a background variable—it is, increasingly, a defining feature of bladder cancer behaviour and treatment response. Prognostic risk tables developed for high risk bladder tumour recurrence should emphasize a UTUC history, as it portends a poorer clinical outcome in addition to conventional clinicopathological features. More importantly, while we are witnessing a burgeoning body of evidence supporting bladder-preserving strategies for BCG-unresponsive disease, their clinical applicability and outcomes in M-NMIBC will need to be interpreted with caution.
Written by: Dr. Yu Guang Tan,1 Dr. Benjamin Jia Han Lim,1 Dr. Tsung Wen Chong,1 Dr. Kenneth Chen,1 Dr. Kae Jack Tay,1 Dr. John SP Yuen,1 Dr. Michael R. Abern2- Department of Urology, Singapore General Hospital.
- Department of Urology, Duke University School of Medicine, Durham, NC, USA
References:
- Aragon-Ching, J. B. & Wang, H. Contemporary treatment and survival differences in patients with urothelial versus nonurothelial bladder and upper tract carcinomas: Analyses from the National Cancer Database (NCDB). Journal of Clinical Oncology 40, 463-463, doi:10.1200/JCO.2022.40.6_suppl.463 (2022).
- Lamm, D. (2006). Improving Patient Outcomes: Optimal BCG Treatment Regimen to Prevent Progression in Superficial Bladder Cancer. In European Urology, Supplements (Vol. 5, Issue 10, pp. 654–659). https://doi.org/10.1016/j.eursup.2006.04.008
- Packiam VT, Lamm DL, Barocas DA, et al. An open label, single-arm, phase II multicenter study of the safety and efficacy of CG0070 oncolytic vector regimen in patients with BCG-unresponsive non-muscle invasive bladder cancer: interim results. Urol Oncol Semin Orig Investig. 2018;36:440–447. doi: 10.1016/j.urolonc.2017.07.005.
- Sylvester RJ, van der MEIJDEN AP, Lamm DL. Intravesical bacillus Calmette-Guerin reduces the risk of progression in patients with superficial bladder cancer: a meta-analysis of the published results of randomized clinical trials. J Urol. 2002 Nov;168(5):1964-70. doi: 10.1016/S0022-5347(05)64273-5. PMID: 12394686.
- Fadl-Elmula, I.; Gorunova, L.; Mandahl, N.; Elfving, P.; Lundgren, R.; Mitelman, F.; Heim, S. Cytogenetic monoclonality in multifocal uroepithelial carcinomas: Evidence of intraluminal tumour seeding. Br. J. Cancer 1999, 81, 6–12
- Green DA, Rink M, Xylinas E, Matin SF, Stenzl A, Roupret M, Karakiewicz PI, Scherr DS, Shariat SF. Urothelial carcinoma of the bladder and the upper tract: disparate twins. J Urol. 2013 Apr;189(4):1214-21. doi: 10.1016/j.juro.2012.05.079. Epub 2012 Sep 27. PMID: 23023150.
- Catto JW, Azzouzi AR, Rehman I, Feeley KM, Cross SS, Amira N, et al. Promoter hypermethylation is associated with tumor location, stage, and subsequent progression in transitional cell carcinoma. J Clin Oncol 2005;23(13):2903–10. https://doi.org/10.1200/JCO.2005.03.163.
- Agundez M, Grau L, Palou J, Algaba F, Villavicencio H, Sanchez-Carbayo M. Evaluation of the methylation status of tumour suppressor genes for predicting bacillus Calmette-Guerin response in patients with T1G3 high-risk bladder tumours. Eur Urol 2011;60(1):131–40.
- Breyer J, Wirtz RM, Erben P, et al. High CDKN2A/p16 and low FGFR3 expression predict progressive potential of stage pT1 urothelial bladder carcinoma. Clin Genitourin Cancer