This study developed a prognostic model specialized for patients with mUTUC who received first-line systemic therapy, based on a cohort of 476 patients from Peking University Cancer Hospital (PUCH) spanning nearly two decades (from January 2005 to March 2024). The entire cohort was randomly divided into a development cohort (75%) and a validation cohort (25%). Potential prognostic factors were recorded prospectively. The authors initially assessed the performance of the Bajorin model within the cohort and found that it lacked sufficient discriminatory power to accurately predict outcomes in patients with mUTUC (Fig. 1).
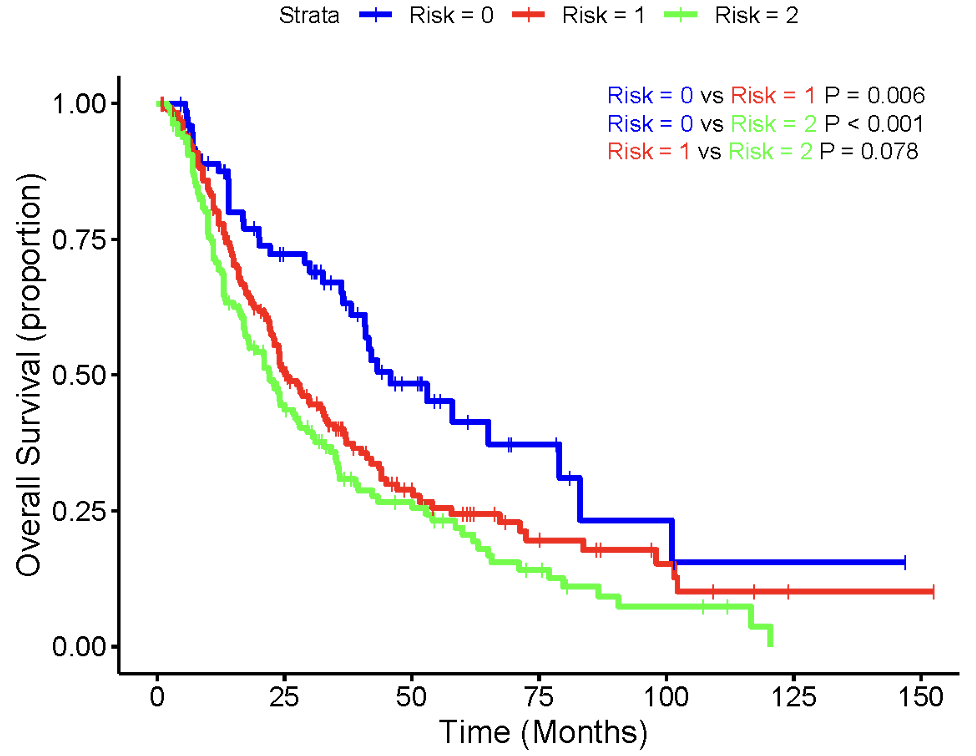
Fig 1. Kaplan-Meier curve based on number of first-line Bajorin risk factors.
They therefore conducted univariate and multivariate analyses in this cohort to identify significant prognostic factors for mUTUC and revealed five independent risk factors:
- Number of metastatic organs ≥3 (hazard ratio [HR] 1.41, 95% confidence interval [CI] 1.04–1.91).
- Eastern Cooperative Oncology Group (ECOG) performance status >1 (HR 2.28, 95% CI 1.30–3.97).
- Time to distant metastasis (TTDM) <12 months (HR 3.01, 95% CI 2.13–4.26).
- White blood cell (WBC) count > upper limit of normal (ULN) (HR 1.89, 95% CI 1.21–2.95).
- Alkaline phosphatase (ALP) > ULN (HR 1.71, 95% CI 1.10–2.64).
They further developed a new prognostic model (PKUCH model), assigning one point to each independent risk factor and categorizing patients into three risk groups in the development cohort (P < 0.001, Fig. 2):
- Favorable (0 risk factors): median overall survival (mOS) of 65.0 months (95% CI 12.1–19.9).
- Intermediate (1 risk factor): mOS of 32.0 months (95% CI 25.8–38.2).
- Poor (2+ risk factors): mOS of 16.0 months (95% CI 12.1–19.9).

Fig 2. Kaplan-Meier curve for each risk group (0, 1, or 2+ risk factors) in development cohort of this study.
The c-statistic was 0.71 in the development cohort and 0.72 in the validation cohort, among the highest reported for first-line mUC prognostic models by far (Fig. 3).
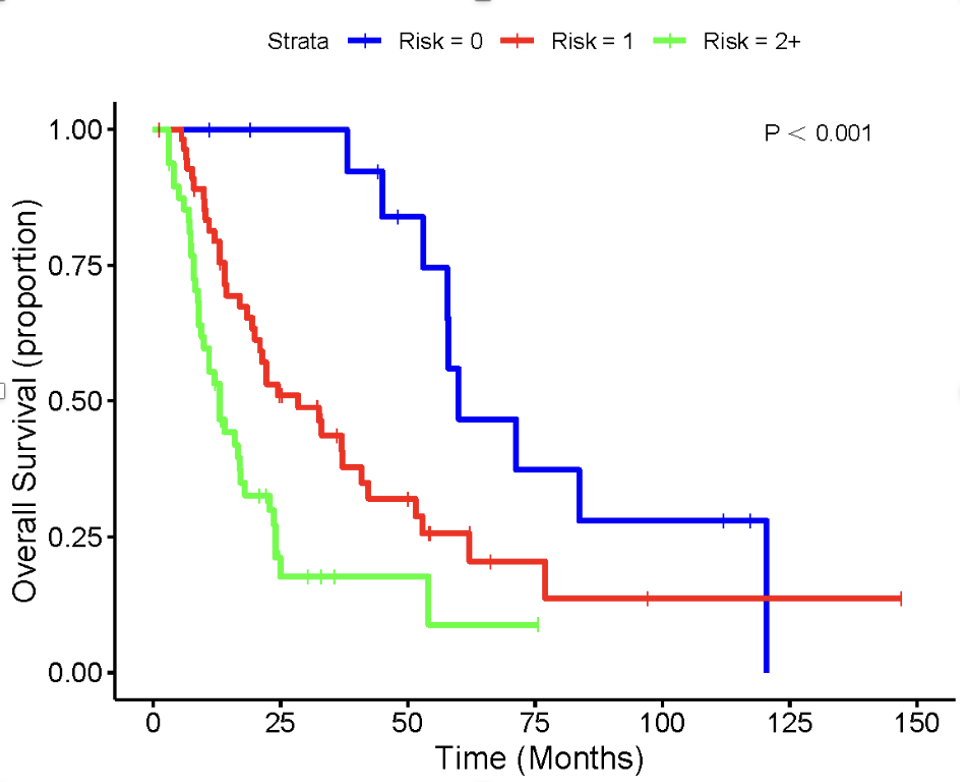
Fig 3. Kaplan-Meier curve for each risk group (0, 1, or 2+ risk factors) in validation cohort of this study.
As a supplementary result, a nomogram was developed based on these prognostic factors to predict 1-, 2-, and 5-year OS probabilities for individual patients, taking into account the HRs of the identified prognostic factors (Fig. 4).
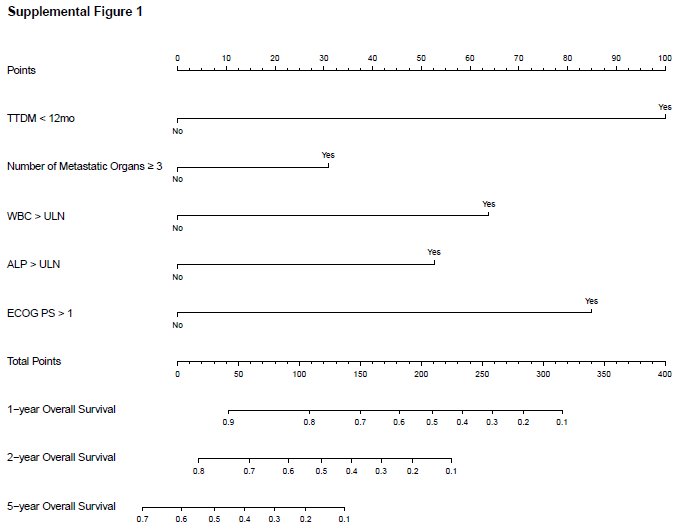
Fig 4. Calibration curve of final nomogram.
This is the first prognostic model specifically designed for patients with mUTUC receiving first-line systemic therapy. This model offers a much-needed tool for clinicians to predict outcomes prior to initiating first-line chemotherapy, enabling the stratification of patients and more informed treatment decisions, with the potential to improve patient management in real-world clinical settings.
Written by: Xinan Sheng, Department of Genitourinary Oncology, Peking University Cancer Hospital & Institute, Beijing, China.