
Advancing Biomarker-Based Diagnostics in Small Testicular Masses
With the increased use of high-resolution testicular ultrasonography, urologists are identifying a growing number of small testicular masses (STMs ≤ 2 cm). While most are benign, the inability to distinguish them reliably from malignant lesions often leads to unnecessary orchiectomies. Conventional serum markers (AFP, β-hCG, LDH) have limited sensitivity for early disease, reinforcing the need for better molecular tools.
In our recently published work in European Urology Oncology, we evaluated circulating microRNAs (miRNAs) as minimally invasive biomarkers to detect malignancy in patients with STMs. Serum and plasma samples from 61 patients with histologically confirmed lesions across three international laboratories. Among all miRNAs evaluated (miR-367, miR-371, miR-372, miR-373), miR-371a-3p showed the highest diagnostic performance, with a sensitivity of 87%, specificity of 91%, and an AUC of 0.93.
As shown in the figure below, receiver operating characteristic (ROC) curves demonstrated reproducible results across laboratories, Vancouver (RT-qPCR plasma, AUC = 0.943), Porto (RT-qPCR serum, AUC = 0.786), and Toronto (ddPCR serum, AUC = 0.745), highlighting consistency across both platform and biospecimen type.

The table below further details optimal cut-off points and performance metrics for individual miRNAs, underscoring that miR-371a-3p consistently outperformed miR-367, miR-372, and miR-373 in sensitivity and specificity across all centers. These findings confirm miR-371a-3p as a robust, reproducible biomarker for malignancy detection in STMs.
Table: Optimal cutoffs and performance characteristics of different miRNAs

Methodological Development: Standardizing miRNA Quantification
As detailed in the table below, our project involved three participating laboratories: Vancouver, Toronto, and Portugal, each employing distinct extraction and quantification pipelines to evaluate circulating miRNAs. The Vancouver and Toronto sites used plasma and serum samples, respectively, with column-based or plasma extraction kits (QIAGEN miRNeasy Serum/Plasma), while the Portuguese laboratory utilized a magnetic bead–based platform (MagMAX™ miRVana). These methodological differences extended to preamplification conditions, normalization controls (hsa-miR-30b-5p), and spike-in references (cel-miR-39-3p or ath-miR-159a).
Two main analytical platforms were compared: digital droplet PCR (ddPCR) and reverse transcription quantitative PCR (RT-qPCR) with preamplification. Both approaches demonstrated strong performance when evaluating the total miRNA population, showing robust reproducibility and clear discrimination between benign and malignant cases. In contrast, assays focused on extracellular vesicle (EV)-enriched fractions were more technically variable and yielded inconsistent results, underscoring the challenges of isolating EV-specific miRNAs in a clinical setting.
This multi-laboratory comparison not only highlights the feasibility of standardizing miRNA-based assays across international sites but also provides insight into how analytical nuances such as extraction chemistry, input volume, and quantification methodology can influence biomarker performance. Collectively, these findings lay the groundwork for the harmonization of miRNA testing protocols, ensuring consistency and reliability as these biomarkers move toward clinical validation.
Table: Summary of different laboratory pipelines and methodology for miRNA extraction

Ongoing Prospective Study: Biomarker-Guided Management
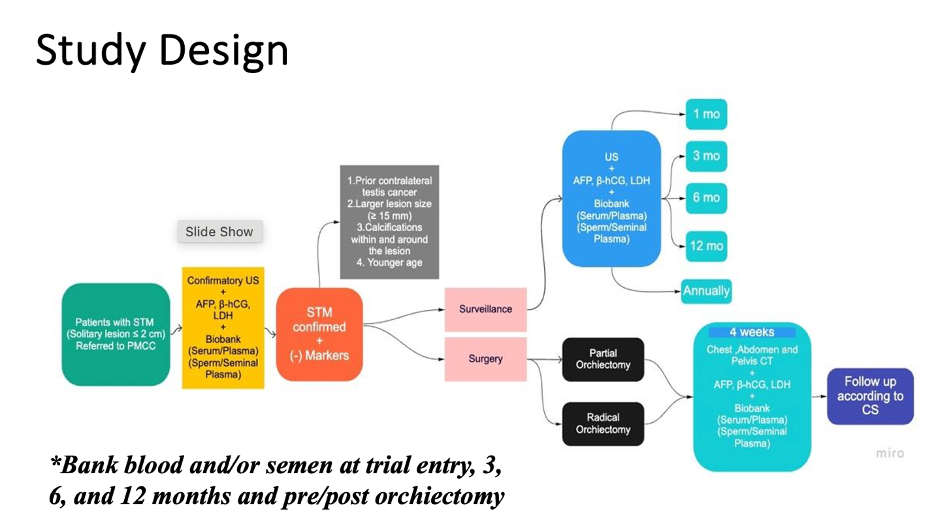
Building on these findings, we are now conducting a prospective biomarker-driven trial to determine whether surveillance can safely be offered to patients with biomarker-negative STMs. The trial design, shown in the figure below, outlines a structured pathway beginning with confirmatory ultrasound and conventional serum markers, followed by optional surgery or surveillance based on histologic and biomarker results. Eligible patients with solitary lesions ≤ 2 cm undergo serial imaging and biobanking of serum, plasma, and seminal plasma at entry, 3, 6, and 12 months, as well as pre- and post-orchiectomy.
This longitudinal design aims to capture real-time biomarker dynamics, validating whether persistently negative miR-371a-3p levels can safely identify candidates for observation rather than immediate surgery. The trial also enables correlative analyses between miRNA trends, imaging evolution, and histopathology, laying the groundwork for biomarker-guided decision-making in clinical practice.
Looking Ahead
Together, these complementary efforts, the international validation of miR-371a-3p, the ongoing prospective surveillance trial, and the methodological standardization initiative represent a major advance toward biomarker-guided management of small testicular masses. By uniting expertise across continents and disciplines, this collaboration is bridging the gap between molecular discovery and real-world clinical practice, with the potential to shift STM management from surgical default to precision surveillance for biomarker-negative patients.
Lastly, we would like to acknowledge the generous support of the Princess Margaret Agnico-Eagle Early Detection Grand Challenge Grant, the University of Toronto Hold’em for Life Oncology Fellowship Grant, and the Princess Margaret Cancer Foundation for their continued support of these projects. Their contributions have been instrumental in advancing our ongoing efforts to develop biomarker-driven strategies for the diagnosis and management of small testicular masses.
Written by: Julian Chavarriaga, MD, Urologic Oncologist, Penn State Health, Hershey, PA
Read the Abstract